
akn
Musclechemistry Member
by Mike Arnold
Out of all the side effects a steroid user could potentially experience, gynecomastia (aka bitch tits) is one of the worst…and it certainly tops the list when it comes to cosmetic side effects. Being heavily associated with womanhood, the very nature of this side effect is an affront to our masculinity. Not only is it embarrassing, but in some cases it can destroy the entire appearance of one’s physique. We have all seen pictures of the more extreme cases, where the BB’r literally looks like he has grown a small pair of tits on an otherwise normal body. The severity of this condition can range from only slight swelling, which is often imperceptible from a visual standpoint, to the more extreme cases, as mentioned above Fortunately, gynecomastia does not develop over night and its progression is easily halted and reversed if the proper steps are taken in a timely fashion. There really isn’t any good excuse for a steroid user to experience permanent, visible breast tissue growth. Those that do either don’t care or rather (and much more likely), they weren’t prepared and/or educated to deal with this side effect ahead of time. While there are numerous potential causes of this condition, the BB’r generally only has to worry about a few of them and the available treatment options are simple in their application. Through minimal self-education and a small financial investment we have all the tools we need to keep this side effect at bay.
Why are my nipples sore?
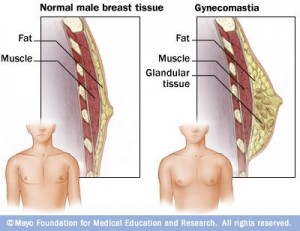
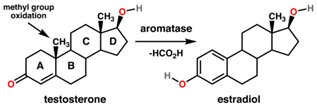
The most important factor in the prevention of gyno is knowing how it occurs in the first place. Since this article is targeted mainly towards the steroid-using BB’r, we will only address the causes which are directly attributable to PED usage. There are 4 types of steroids which can cause gynecomastia , the most prominent of which are the aromatizable steroids. Aromatizable steroids are those AAS which are capable of converting to estrogen. This includes many steroids, such as testosterone, methyltestosterone, methandrostanolone (Dianabol), and to a lesser degree, nandrolone (Deca/NPP), and boldenone (EQ). This conversion process is initiated when aromatizable AAS interact with aromatase, which is an enzyme necessary for the biosynthesis of estrogen. See below for a depiction of this interaction:
When low dosages of these steroids are administered, the degree of conversion is not sufficient to cause this side effect. However, this threshold is regularly crossed by BB’rs who utilize dosages well in excess of those required to avoid estrogenic side effects. The problem with being able to pin-point the dose at which this side effect occurs is that not all individuals are affected equally by the same dose. Some can get away with using fairly large dosages of highly aromatizing drugs, such as testosterone, while others seem to develop problems even with minimal use. I know a powerlifter who was able to use a full gram of pharmaceutical-grade testosterone per week without experiencing any gyno symptoms, while other people have encountered early signs of gynecomastia at only 250 mg weekly. For this reason, assumptions should not be made beforehand regarding personal tolerance. When it comes to learning your limit, real-world experience must be your teacher. However, if I had to guess, I would say that most individuals will begin to experience the early stages of gyno by the time they reach 400-500 mg per week when using testosterone, assuming preventative action is not taken.
The 2nd type of steroid which can potentially cause gyno are those which appear to exhibit inherent estrogenic activity, despite lacking the ability to aromatize. One example would be oxymetholone (Anadrol). This steroid is not capable of converting to estrogen to any degree, yet it causes gyno in a moderate percentage of users. The most plausible explanation for this side effect is that the Anadrol molecule itself demonstrates estrogenic activity, likely by attaching directly to the estrogen receptor. While we cannot yet conclusively state this to be fact, it seems more probable than the other theories which have been put forward over the years.
The 3rd type of AAS associated with the development of gynecomastia are the progestin-based steroids, which promote their effects through direct stimulation of the progesterone receptor. Two examples which fit this description would be trenbolone and nandrolone. However, these drugs differ from the previously mentioned AAS in that they rarely cause gyno on their own. Typically, they require the presence of estrogen (usually at above normal levels) in order to have an impact on the growth of breast tissue. In essence, their progestagenic effects tend to exacerbate the effect of estrogen, thereby acting more as a contributor rather than the primary offender.
The last category of AAS with a history of exhibiting this side effect are those which result in estrogen-rebound. Anticipating the effects of these drugs can be difficult, as they are much less predictable in their behavior. Not only does personal response vary tremendously between individuals, but there is often a lack of consistency even among the same individual. For example, a particular steroid may be employed multiple times without incident, only to cause troubling gyno symptoms under nearly identical circumstances at a later date.
We’ve looked at particular types of AAS and how they work to cause gyno, but there are other causes which should not be overlooked, one of which is an out of balance androgen to estrogen ratio. DHT itself, as well as many DHT derivatives, possess natural anti-estrogenic activity. Therefore, even in the face of stable estrogen levels, a reduction in these hormones may lead to the appearance of estrogenic side effects. In turn, an increase in DHT or its related metabolites will enable an individual to more effectively deal with increased levels of estrogen. This is why a steroid user is much more likely to encounter estrogenic side effects using testosterone alone, compared to a combination of testosterone and drostanolone (Masteron), which was developed specifically for the management of female breast cancer (i.e. Advancement of breast cancer is heavily dependent on the availability of estrogen).
The last cause of gyno in the steroid user is prolactinemia, which is an elevation of prolactin levels outside of the normally recognized limits. The most common cause of prolactinemia in the general population is prolactinoma (tumor of the pituitary gland), although this condition can be caused by administering prolactin elevating steroids, such as trenbolone and nandrolone. However, just like progesterone, prolactin rarely causes gyno by itself. This is not because prolactin is not able to accomplish this. Rather, AAS generally aren’t able to elicit elevations in prolactin adequate for causation. Most of the time, prolactin acts to exacerbate the effects of estrogen (similar to progesterone), making it a contributing factor and not the primary cause in the large majority of cases. Still, there have been instances in which these steroids were able to cause gyno and/or lactation independent of aromatizable AAS. I want to emphasize the fact that lactation rarely occurs in steroid users, but when it does, it is almost always attributable to excessive dosing with the offending steroids, in combination with poor personal response.
The Cure
Once you’ve indentified the root of the problem, deciding on the best course of action is relatively simple. With that said, let’s get right to the nuts-n-bolts of how to get rid of gyno. When excess estrogen levels are the culprit (aromatizable AAS), there are multiple treatment methods available to us. Ideally, you want to stop the problem before it even begins. Therefore, when planning your cycle, if you know you will be using a dose of aromatizable drugs likely to raise estrogen into a problematic range, the concomitant administration of an A.I. (anti-aromatase) from the outset of your cycle is the best bet. By making an A.I. an integral component of your program right from the start, you will never find yourself in an emergency situation.
While A.I’s can be used in either the prevention or reversal of gyno symptoms, they are best employed as a preventative measure…and with good reason. You see, the job of an A.I. is to prevent testosterone from aromatizing into estrogen, which it does very well, but the problem is that it does absolutely nothing to prevent currently circulating estrogen from continuing to cause problems. As long as A.I’s are utilized as a preventative measure and not for the treatment of an emergency situation, they are preferable to other gyno remedies, but that is not all. The primary mechanism by which A.I’s inhibit gyno formation (management of systematic estrogen) also provides numerous other benefits not found elsewhere, such as: reduced water retention, lowered blood pressure, decreased fat storage, and others. Lastly, A.I.’ do not reduce IGF-1 levels, as will tamoxifen (Nolvadex).
Should you find yourself in a situation where gyno symptoms manifest unexpectedly, you should turn to tamoxifen (Nolvadex) for assistance. Why? The body is programmed to convert a percentage of our naturally produced testosterone into estrogen. This is a necessary and healthy process, as estrogen is required for a variety of male physiological functions. However, as the dose of androgens continues to rise, the body continues to convert roughly the same amount of androgens into estrogen. This becomes a problem once we begin administering supraphysiological quantities of these drugs. The much greater amounts of estrogen now floating through the bloodstream are free to attach to any estrogen receptor sites they come in contact with, including those in breast tissue. The end result is gyno formation…also known as “growing boobs”. This is great in teenage girls, but not in grown men.
The only way to put an immediate stop to this is by deactivating estrogen in breast tissue. Tamoxifen does just that. Due to its greater binding affinity, Tamoxifen is able to dislocate estrogen from the receptor site and take its place, leaving the estrogen with nowhere to attach. The main downside of Tamoxifen relative to the A.I.’s, aside from its IGF-1 lowering effect, is that it is powerless to reduce systematic estrogen levels. Because whole-body estrogen levels remain elevated, the user is subject to side effects such as water retention, increased fat storage, increased blood pressure, etc.
The 3rd way to treat estrogen-induced gyno is through the use of anti-estrogenic steroids, such as Masteron or Proviron. Of this we can be certain, as Masteron has been proven effective, in a clinical setting, at modulating estrogen levels in breast tissue. In fact, Masteron was originally designed for use in women afflicted with breast cancer. Like A.I.’s, Masteron and gang work to keep estrogen levels low by preventing aromatization. As mentioned above, this is a decisive advantage compared to a drug like Tamoxifen, which is completely ineffective at managing whole-body estrogen. This also means it is best used as a preventative measure and not in emergency situations. As a whole, anti-estrogenic steroids are not as potent as the A.I’s. Therefore, these steroids should be utilized right from the start of a cycle, at a dosage commensurate to the amount of aromatizable drugs being used. In my opinion, Masteron is usually the best steroid for this purpose, as it not only provides an anti-estrogenic punch similar to Proviron, but it also increase the muscle-building value of a cycle, unlike Proviron, which has virtually no muscle building effect. Lastly, Masteron provides the additional benefit of enhanced sex drive.
We’ve spoken a lot on estrogen-induced gyno, but not all gyno is estrogen dependent. Prolactin has the ability to cause gyno if levels get high enough, as does progesterone. While AAS do not directly increase progesterone levels, some steroids themselves are progestins (ex. trenbolone & nandrolone), exhibiting progestagenic effects on the body. Generally, this progestagenic effect is not strong enough to cause gyno by itself, but it can certainly exacerbate the effects of estrogen, making the problem worse. In the same way, AAS are generally not able to increase prolactin high enough in order to cause gyno by itself, yet it can certainly contribute to the problem. In extreme cases, individuals using large doses of Trenbolone have been known to lactate. Although this is rare and typically only occurs in heavy users with an unfavorable response, it does occasionally happen.
The most effective treatment for normalizing prolactin levels are the anti-prolactin drugs, such as cabergoline, pramipexole, or bromocriptine. Bromocriptine is a 1st generation anti-prolactin drug. It is not as potent as the other two and since it is less specific in its actions, it comes with an increased risk of side effects. There is no longer any good reason to choose bromocriptine when seeking relief from elevated prolactin. While cabergoline and pramipexole will both get the job done, in terms of compatibility and ease of use, caber is usually preferred due to its reduced side effect profile and longer active life. If there is one downside, it would be its greater cost. Pramipexole must be dosed daily, while cabergoline is usually only administered once every 2-3 days, depending on need. As for the progestagenic effects of AAS, a stated above, gyno is rarely ever a concern as long as estrogen levels are properly managed. Therefore, no specific treatment is indicated. Rather, you indirectly treat the problem by maintaining a normal estrogen level.
That about sums it up, guys. If there is one take home message here, it is that prevention is preferable to correction. Stop gyno before it starts by keeping your estrogen level stable and it is very unlikely that you will ever have gyno issues. For those who are very sensitive to the effects of prolactin, yet like to use high doses of trenbolone or nandrolone, you may require the additional use of an anti-prolactin drug. However, most of us will not need these in order to avoid gyno.
Obviously, personal experience will play a key role in showing us what we can and cannot do as we attempt to stay gyno-free, so as you go about experimenting with different steroids & dosages, make sure you have the appropriate ancillaries on hand just in case they are needed. It is always wise to have a back-up supply of Tamoxifen lying around, simply because it’s almost universally effective for stopping gyno, regardless of the cause.