
HackTwat
MuscleChemistry Registered Member
IGF-1 LEVELS AND SEXUAL FUNCTION: PART 2 OF 2
.....continued from Part 1.......
Subjects' IGF-1 levels were also correlated with self-reported sexual function as assessed using the sexual and hormonal domains of the EPIC questionnaire. The median±s.d. score of the sexual domain of the EPIC questionnaire was 56.4±28.3 (range 6.3–96.2) (). Similar to the findings with SHIM score, there was a significant correlation between the sexual domain of the EPIC questionnaire and IGF-1 levels for all ages ( r=0.30, P=0.02) (, Figure 2). In contrast, there was no correlation between the sexual domain of the EPIC questionnaire and IGF-1 levels for any single age group, although the correlation within the >70-year-old age group approached significance ( r=0.87, P=0.06). In addition, no significant correlation was found between testosterone level and SHIM or EPIC score, which supports previous findings in the literature. [SUP][32][/SUP] In addition, there was no correlation between the hormonal domain of the EPIC questionnaire and either IGF-1 or testosterone levels.
Table 1. Patient characteristics
<TBODY>
</TBODY>Abbreviations: BMI, body mass index; ED, erectile dysfunction; EPIC, Expanded Prostate Cancer Index Composite; IGF-1, insulin-like growth factor 1; RP, radical prostatectomy; SHIM, Sexual Health Inventory for Men; TRT, testosterone replacement therapy.
Table 2. Spearman's correlation coefficients between IGF-1 and SHIM/EPIC scores, IGF-1 and testosterone, by age
<TBODY>
</TBODY>Abbreviations: IGF-1, insulin-like growth factor 1; EPIC, Expanded Prostate Cancer Index Composite; SHIM, Sexual Health Inventory for Men. 'R' represents the Spearman's correlation coefficient. 'EPIC sex' refers to the sexual domain portion of the EPIC questionnaire, whereas 'EPIC horm' refers to the hormonal domain. SHIM 1—SHIM 5 refer to individual questions of the SHIM questionnaire.
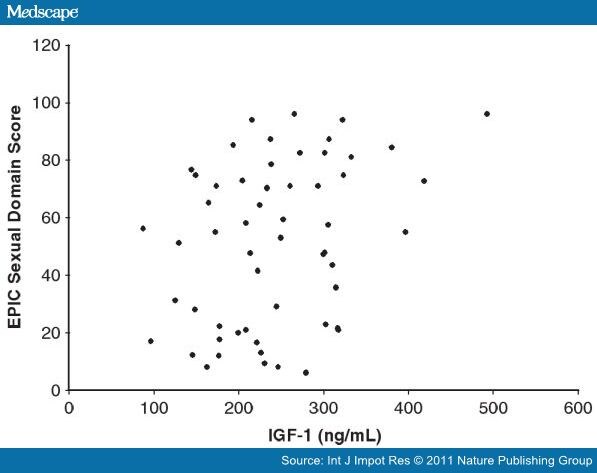
Figure 2.
Total Expanded Prostate Cancer Index Composite (EPIC) sexual domain score vs serum insulin-like growth factor 1 (IGF-1) Level. All subjects' IGF-1 level plotted against their self-reported scores of sexual function based on the sexual domain portion of the EPIC questionnaire. There is a statistically significant correlation between the two measured values (Spearman's correlation coefficient, r=0.30; P=0.02).
To control for the impact of comorbidities on IGF-1 levels, multivariate analysis using linear regression modeling was carried out. These data demonstrated that only hyperlipidemia is predictive of IGF-1 levels ( P=0.02, ), with other comorbidities not significantly impacting IGF-1 levels. The prevalence of hyperlipidemia in our subject population as a function of age revealed no significant difference, suggesting that the presence of hyperlipidemia does not affect the findings described above.
Table 3. Multivariate analysis assessing IGF-1 levels, age and comorbidities
<TBODY>
</TBODY>Abbreviation: IGF-1, insulin-like growth factor 1
In light of reports suggesting that elevated IGF-1 and GH levels stimulate prostate cancer cell growth, we determined the Spearman's rank correlation between IGF-1 level and both total Gleason score, as well as the high component of the Gleason score. Our data demonstrate no significant correlation between IGF-1 levels and Gleason score, suggesting that while GH and IGF-1 may stimulate the growth of prostate cancer, tumor severity is not affected in this group of men scheduled for radical prostatectomy. In addition, no correlation was shown between testosterone level and Gleason score for all ages or in any age group (data not shown).
Discussion
The prevalence of LOH is likely to continue increasing as the world's population ages. Recent work has established a role for testosterone in the development and maintenance of erections, and testosterone replacement has been shown to ameliorate the symptoms of LOH, including erectile dysfunction. [SUP][33–35][/SUP] In contrast, the role of GH in the maintenance of sexual function is less well established, although studies have shown a relationship between GH and erectile function.
In this work, we demonstrate a statistically significant correlation between self-reported, validated measures of sexual function in men, the SHIM and EPIC questionnaires, and IGF-1 levels, most robustly in men >70, as well as in men between 50 and 59 years old. In contrast, a correlation between testosterone levels and SHIM/EPIC scores is not demonstrated. Notably, study subjects were given SHIM and EPIC questionnaires after a diagnosis of prostate cancer had been made. Given the psychologically stressful nature of a cancer diagnosis, this may have resulted in lower SHIM and EPIC scores. However, given that all men in the study carried the diagnosis of prostate cancer, a uniform reduction in questionnaire scores would be expected, a possibility we cannot evaluate given the lack of pre-diagnosis questionnaire responses.
Erectile dysfunction is a known early predictor of coronary artery disease. Deficiency of GH or IGF-1 has been implicated in the pathogenesis of cardiovascular disease and atherosclerosis and is associated with an increased prevalence of ischemic heart disease. [SUP][16,17][/SUP] GH/IGF-1 deficiency is thought to contribute to endothelial dysfunction, and low GH/IGF-1 levels have been correlated with a decreased number and diminished function of endothelial progenitor cells, which function in vascular repair. [SUP][27][/SUP] Notably, this endothelial progenitor cell dysfunction is reversible with GH administration, which suggests a possible role for GH in the treatment of vascular disorders, including erectile dysfunction. [SUP][27][/SUP] GH and IGF-1 have also been shown to have antioxidant and anti-inflammatory effects in animal models, suggesting a protective role for GH/IGF-1 in vascular disease given the role of oxidative stress in initiating lipid-lesion formation as well as in the destabilization and progression of these lesions. [SUP][36][/SUP] Interestingly, our data link IGF-1 levels to hyperlipidemia, highlighting a potential interplay between serum lipids and GH/IGF-1 levels. Although it is tempting to hypothesize that this correlation may indicate a response by the GH axis to hyperlipidemia, additional analysis is necessary to fully elucidate this.
GH has been shown to modulate the NO/cyclic guanosine monophosphate signaling pathways and aid in the restoration of cavernosal smooth muscle integrity in rats. [SUP][24][/SUP] GH levels increase during sexual arousal and GH has been shown to induce relaxation of smooth muscle in a dose-dependent manner and upregulate NO and cyclic guanosine monophosphate serum levels in human corpus cavernosum. [SUP][20,29][/SUP] GH has also been shown to have a trophic effect on neuronal and endothelial nitric oxide synthase- (nNOS and eNOS, respectively) containing neurons after cavernous neurotomy in rats, suggesting that GH may be important in the maintenance or restoration of erectile function post-prostatectomy. [SUP][23][/SUP] Like, GH, IGF-1 has growth-stimulating effects and is thought to improve erectile function in diabetic rats as measured by maximum intracavernosal pressure as well as the maximal intracavernosal pressure to mean arterial pressure ratio. [SUP][22,37][/SUP] Together these data support a role for GH and IGF-1 in sexual arousal and erectile function, and indicate that GH and IGF-1 may function using a well-established pathway for erectile stimulation.
A relationship between GH, IGF-1 and testosterone has previously been demonstrated. [SUP][1,2][/SUP] Curiously, no significant correlation is demonstrated between serum IGF-1 and testosterone levels or between testosterone levels and SHIM/EPIC scores in our work. However, we have observed this correlation to be lacking in patients seen in our practice that were not included in this study, and suspected that this finding may be related to the use of exogenous testosterone by patients before presentation to our clinic, which would affect serum testosterone levels and could affect the relationship between testosterone and IGF-1.
In light of our findings linking the GH axis to sexual dysfunction, it is conceivable that supplementation with GH or IGF-1 could improve recovery of erectile function after radical prostatectomy. However, there is concern regarding a possible role for GH, IGFs and IGF-binding proteins (IGFBPs) in the development of prostate cancer and stimulation of its growth. [SUP][26][/SUP] GH has been shown to stimulate prostate cancer cell growth and both GH and the GH receptor is expressed in prostate cancer cells, suggesting a potential auto- or paracrine pathway for stimulating growth. [SUP][38][/SUP] Elevated IGF-1 levels, as well as low IGFBP3 levels, were recently shown to correlate with an up to 21% increased risk of prostate cancer, and an increased risk of prostate cancer has been demonstrated in Latin men with elevated IGF-1 levels, results that have been echoed in other cohorts. [SUP][39–41][/SUP] These data argue for caution when considering supplementation with GH or IGF-1 in men with erectile dysfunction.
In this study, we found no correlation between Gleason score and IGF-1 levels. Although this does not suggest that GH does not stimulate prostate cancer cell growth, the data argue that the GH axis does not stimulate development of more aggressive tumors. However, whether men being treated with GH have an increased risk of prostate cancer and whether exogenous GH administration affects tumor severity cannot be addressed. Further work defining the mechanisms of function of GH and IGF-1 in prostate cells should be undertaken and the risks of carcinogenesis should be more clearly defined. In addition to the lack of correlation between serum IGF-1 levels and Gleason score, no significant correlation was identified between serum testosterone levels and Gleason score. Although a link between serum testosterone levels and prostate cancer severity has been demonstrated, previous studies have focused on Gleason scores ≥8 and found an increased risk of more aggressive prostate cancer only in men ≥65 years old. [SUP][42][/SUP] In our analysis, only four patients had Gleason score 8 or higher cancer and only one of these was more than 65 years old, which may explain a lack of correlation between serum testosterone level and Gleason score given the predominance of Gleason score 6 and 7 prostate cancer within our cohort. However, in a recent study of 478 men screened for prostate cancer with transrectal ultrasound-guided biopsy, no relationship was observed between serum testosterone level and prostate cancer severity. [SUP][43][/SUP] Thus, it is possible that the relationship between testosterone level and Gleason score is indeed most significant in older men with more aggressive tumors.
Our study was limited by several factors. First, the study was performed with a cohort of men diagnosed with prostate cancer. Although the considerations for questionnaire score are addressed above, it is also possible that unaccounted for factors, including individual differences in anxiety levels before major surgery or as a result of the cancer diagnosis, may have affected both IGF-1 levels and erectile function. Second, most of the correlations, save for those in the >70-year-old age group, are fairly low. Although this could be a result of the factors above, there may be additional variables that affect the relationship between the GH axis and sexual function and are currently unaccounted for.
Considering the overlap between GH and testosterone in the pathogenesis of erectile dysfunction, it may be beneficial to evaluate both the testosterone and GH axes when evaluating etiology and considering the treatment of erectile dysfunction. Our results support a relationship between IGF-1 and male sexual function, and strengthen the argument to more closely study the role of IGF-1 in erectile dysfunction. There do not exist sufficient data to use IGF-1 or GH supplementation in men with erectile dysfunction currently, and studies demonstrating a role of GH and IGF-1 in development and progression of prostate cancer may further temper this possibility. However, recent studies, including ours, show potential and promise for new ways to enhance current treatment protocols that could improve quality of life in men with erectile dysfunction.
References
<!-- article content ends here -->
.....continued from Part 1.......
Subjects' IGF-1 levels were also correlated with self-reported sexual function as assessed using the sexual and hormonal domains of the EPIC questionnaire. The median±s.d. score of the sexual domain of the EPIC questionnaire was 56.4±28.3 (range 6.3–96.2) (). Similar to the findings with SHIM score, there was a significant correlation between the sexual domain of the EPIC questionnaire and IGF-1 levels for all ages ( r=0.30, P=0.02) (, Figure 2). In contrast, there was no correlation between the sexual domain of the EPIC questionnaire and IGF-1 levels for any single age group, although the correlation within the >70-year-old age group approached significance ( r=0.87, P=0.06). In addition, no significant correlation was found between testosterone level and SHIM or EPIC score, which supports previous findings in the literature. [SUP][32][/SUP] In addition, there was no correlation between the hormonal domain of the EPIC questionnaire and either IGF-1 or testosterone levels.
Table 1. Patient characteristics
| Variable | % (x/n) |
|---|---|
| Median age, years (range) | 58 (46–77) |
| Age | |
| <50 years | 6.2 (4/65) |
| 50–59 years | 49.2 (32/65) |
| 60–69 years | 33.8 (22/65) |
| >70 years | 10.8 (7/65) |
| Race | |
| White or Caucasian | 85.2 (23/27) |
| Black | 11.1 (3/27) |
| Hispanic | 3.7 (1/27) |
| Comorbid conditions | |
| Diabetes mellitus | 13.8 ( 9/65) |
| Hypertension | 41.5 (27/65) |
| Hyperlipidemia | 46.2 (30/65) |
| Coronary artery disease | 4.6 (3/65) |
| Depression | 6.2 (4/65) |
| Social history | |
| Cigarette smoking | |
| Non-smoker | 75.4 (49/65) |
| Previous history of smoking | 21.5 (14/65) |
| Current smoker | 3.1 (2/65) |
| Occasional to moderate alcohol consumption | 49.2 (32/65) |
| Sexual history | |
| ED before RP | 29.2 (19/65) |
| TRT before RP | 3.1 (2/65) |
| Mean BMI, n (range) | 27.6, 11 (20.0–37.8) |
| Prostate cancer Gleason grade | |
| 3 + 3 | 56.9 (33/58) |
| 3 + 4 | 27.6 (16/58) |
| 4 + 3 | 6.9 (4/58) |
| 4 + 4 | 3.4 (2/58) |
| 3 + 6 | 1.7 (1/58) |
| 4 + 5 | 1.7 (1/58) |
| Hormone levels | |
| Median total testosterone (ng dl [SUP]−1[/SUP]), s.d. | 358.0±136.4 |
| Median IGF-1 (mg dl [SUP]−1[/SUP]), s.d. | 235.0±86.4 |
| Questionnaire scores | |
| Median SHIM score, s.d. | 19.5±8.7 |
| Median EPIC sexual score, s.d. | 56.4±28.3 |
| Median EPIC hormonal score, s.d. | 10.0±1.5 |
<TBODY>
</TBODY>
Table 2. Spearman's correlation coefficients between IGF-1 and SHIM/EPIC scores, IGF-1 and testosterone, by age
| Age group | IGF-1 vs | R | P-value |
|---|---|---|---|
| All ages | Total SHIM | 0.31 | 0.02 |

| SHIM 1 | 0.33 | 0.01 |
|
| SHIM 2 | 0.30 | 0.02 |
|
| SHIM 3 | 0.28 | 0.03 |
|
| SHIM 4 | 0.26 | 0.04 |
|
| SHIM 5 | 0.25 | 0.05 |
|
| EPIC sex | 0.30 | 0.02 |
|
| EPIC horm | −0.16 | 0.21 |
|
| Testosterone | −0.03 | 0.84 |
| >70 years | Total SHIM | 0.89 | 0.04 |
|
| SHIM 1 | 0.74 | 0.15 |
|
| SHIM 2 | 0.95 | 0.01 |
|
| SHIM 3 | 0.95 | 0.01 |
|
| SHIM 4 | 0.94 | 0.02 |
|
| SHIM 5 | 0.97 | 0.01 |
|
| epic sex | 0.87 | 0.06 |
|
| EPIC horm | 0.46 | 0.43 |
|
| Testosterone | 0.56 | 0.20 |
| 60–69 years | Total SHIM | 0.26 | 0.26 |
|
| SHIM 1 | 0.41 | 0.07 |
|
| SHIM 2 | 0.10 | 0.66 |
|
| SHIM 3 | 0.18 | 0.43 |
|
| SHIM 4 | 0.18 | 0.43 |
|
| SHIM 5 | 0.17 | 0.47 |
|
| EPIC sex | 0.19 | 0.41 |
|
| EPIC horm | −0.29 | 0.20 |
|
| Testosterone | 0.12 | 0.59 |
| 50–59 years | Total SHIM | 0.33 | 0.09 |
|
| SHIM 1 | 0.31 | 0.10 |
|
| SHIM 2 | 0.41 | 0.02 |
|
| SHIM 3 | 0.29 | 0.12 |
|
| SHIM 4 | 0.23 | 0.22 |
|
| SHIM 5 | 0.22 | 0.24 |
|
| EPIC sex | 0.32 | 0.08 |
|
| EPIC horm | −0.20 | 0.30 |
|
| Testosterone | −0.21 | 0.26 |
| 40–49 years | Total SHIM | −0.74 | 0.26 |
|
| SHIM 1 | −0.89 | 0.11 |
|
| SHIM 2 | NA | NA |
|
| SHIM 3 | −0.26 | 0.74 |
|
| SHIM 4 | NA | NA |
|
| SHIM 5 | NA | NA |
|
| EPIC sex | 0.32 | 0.68 |
|
| EPIC horm | 0.40 | 0.60 |
|
| Testosterone | 0.40 | 0.60 |
<TBODY>
</TBODY>
Figure 2.
Total Expanded Prostate Cancer Index Composite (EPIC) sexual domain score vs serum insulin-like growth factor 1 (IGF-1) Level. All subjects' IGF-1 level plotted against their self-reported scores of sexual function based on the sexual domain portion of the EPIC questionnaire. There is a statistically significant correlation between the two measured values (Spearman's correlation coefficient, r=0.30; P=0.02).
To control for the impact of comorbidities on IGF-1 levels, multivariate analysis using linear regression modeling was carried out. These data demonstrated that only hyperlipidemia is predictive of IGF-1 levels ( P=0.02, ), with other comorbidities not significantly impacting IGF-1 levels. The prevalence of hyperlipidemia in our subject population as a function of age revealed no significant difference, suggesting that the presence of hyperlipidemia does not affect the findings described above.
Table 3. Multivariate analysis assessing IGF-1 levels, age and comorbidities
|
| P-value |
|---|---|
| Age | 0.22 |
| Testosterone | 0.92 |
| Diabetes mellitus | 0.31 |
| Hypertension | 0.80 |
| Hyperlipidemia | 0.02 |
| Coronary artery disease | 0.17 |
| Smoking | 0.63 |
| Alcohol | 0.64 |
| Depression | 0.22 |
<TBODY>
</TBODY>
In light of reports suggesting that elevated IGF-1 and GH levels stimulate prostate cancer cell growth, we determined the Spearman's rank correlation between IGF-1 level and both total Gleason score, as well as the high component of the Gleason score. Our data demonstrate no significant correlation between IGF-1 levels and Gleason score, suggesting that while GH and IGF-1 may stimulate the growth of prostate cancer, tumor severity is not affected in this group of men scheduled for radical prostatectomy. In addition, no correlation was shown between testosterone level and Gleason score for all ages or in any age group (data not shown).
Discussion
The prevalence of LOH is likely to continue increasing as the world's population ages. Recent work has established a role for testosterone in the development and maintenance of erections, and testosterone replacement has been shown to ameliorate the symptoms of LOH, including erectile dysfunction. [SUP][33–35][/SUP] In contrast, the role of GH in the maintenance of sexual function is less well established, although studies have shown a relationship between GH and erectile function.
In this work, we demonstrate a statistically significant correlation between self-reported, validated measures of sexual function in men, the SHIM and EPIC questionnaires, and IGF-1 levels, most robustly in men >70, as well as in men between 50 and 59 years old. In contrast, a correlation between testosterone levels and SHIM/EPIC scores is not demonstrated. Notably, study subjects were given SHIM and EPIC questionnaires after a diagnosis of prostate cancer had been made. Given the psychologically stressful nature of a cancer diagnosis, this may have resulted in lower SHIM and EPIC scores. However, given that all men in the study carried the diagnosis of prostate cancer, a uniform reduction in questionnaire scores would be expected, a possibility we cannot evaluate given the lack of pre-diagnosis questionnaire responses.
Erectile dysfunction is a known early predictor of coronary artery disease. Deficiency of GH or IGF-1 has been implicated in the pathogenesis of cardiovascular disease and atherosclerosis and is associated with an increased prevalence of ischemic heart disease. [SUP][16,17][/SUP] GH/IGF-1 deficiency is thought to contribute to endothelial dysfunction, and low GH/IGF-1 levels have been correlated with a decreased number and diminished function of endothelial progenitor cells, which function in vascular repair. [SUP][27][/SUP] Notably, this endothelial progenitor cell dysfunction is reversible with GH administration, which suggests a possible role for GH in the treatment of vascular disorders, including erectile dysfunction. [SUP][27][/SUP] GH and IGF-1 have also been shown to have antioxidant and anti-inflammatory effects in animal models, suggesting a protective role for GH/IGF-1 in vascular disease given the role of oxidative stress in initiating lipid-lesion formation as well as in the destabilization and progression of these lesions. [SUP][36][/SUP] Interestingly, our data link IGF-1 levels to hyperlipidemia, highlighting a potential interplay between serum lipids and GH/IGF-1 levels. Although it is tempting to hypothesize that this correlation may indicate a response by the GH axis to hyperlipidemia, additional analysis is necessary to fully elucidate this.
GH has been shown to modulate the NO/cyclic guanosine monophosphate signaling pathways and aid in the restoration of cavernosal smooth muscle integrity in rats. [SUP][24][/SUP] GH levels increase during sexual arousal and GH has been shown to induce relaxation of smooth muscle in a dose-dependent manner and upregulate NO and cyclic guanosine monophosphate serum levels in human corpus cavernosum. [SUP][20,29][/SUP] GH has also been shown to have a trophic effect on neuronal and endothelial nitric oxide synthase- (nNOS and eNOS, respectively) containing neurons after cavernous neurotomy in rats, suggesting that GH may be important in the maintenance or restoration of erectile function post-prostatectomy. [SUP][23][/SUP] Like, GH, IGF-1 has growth-stimulating effects and is thought to improve erectile function in diabetic rats as measured by maximum intracavernosal pressure as well as the maximal intracavernosal pressure to mean arterial pressure ratio. [SUP][22,37][/SUP] Together these data support a role for GH and IGF-1 in sexual arousal and erectile function, and indicate that GH and IGF-1 may function using a well-established pathway for erectile stimulation.
A relationship between GH, IGF-1 and testosterone has previously been demonstrated. [SUP][1,2][/SUP] Curiously, no significant correlation is demonstrated between serum IGF-1 and testosterone levels or between testosterone levels and SHIM/EPIC scores in our work. However, we have observed this correlation to be lacking in patients seen in our practice that were not included in this study, and suspected that this finding may be related to the use of exogenous testosterone by patients before presentation to our clinic, which would affect serum testosterone levels and could affect the relationship between testosterone and IGF-1.
In light of our findings linking the GH axis to sexual dysfunction, it is conceivable that supplementation with GH or IGF-1 could improve recovery of erectile function after radical prostatectomy. However, there is concern regarding a possible role for GH, IGFs and IGF-binding proteins (IGFBPs) in the development of prostate cancer and stimulation of its growth. [SUP][26][/SUP] GH has been shown to stimulate prostate cancer cell growth and both GH and the GH receptor is expressed in prostate cancer cells, suggesting a potential auto- or paracrine pathway for stimulating growth. [SUP][38][/SUP] Elevated IGF-1 levels, as well as low IGFBP3 levels, were recently shown to correlate with an up to 21% increased risk of prostate cancer, and an increased risk of prostate cancer has been demonstrated in Latin men with elevated IGF-1 levels, results that have been echoed in other cohorts. [SUP][39–41][/SUP] These data argue for caution when considering supplementation with GH or IGF-1 in men with erectile dysfunction.
In this study, we found no correlation between Gleason score and IGF-1 levels. Although this does not suggest that GH does not stimulate prostate cancer cell growth, the data argue that the GH axis does not stimulate development of more aggressive tumors. However, whether men being treated with GH have an increased risk of prostate cancer and whether exogenous GH administration affects tumor severity cannot be addressed. Further work defining the mechanisms of function of GH and IGF-1 in prostate cells should be undertaken and the risks of carcinogenesis should be more clearly defined. In addition to the lack of correlation between serum IGF-1 levels and Gleason score, no significant correlation was identified between serum testosterone levels and Gleason score. Although a link between serum testosterone levels and prostate cancer severity has been demonstrated, previous studies have focused on Gleason scores ≥8 and found an increased risk of more aggressive prostate cancer only in men ≥65 years old. [SUP][42][/SUP] In our analysis, only four patients had Gleason score 8 or higher cancer and only one of these was more than 65 years old, which may explain a lack of correlation between serum testosterone level and Gleason score given the predominance of Gleason score 6 and 7 prostate cancer within our cohort. However, in a recent study of 478 men screened for prostate cancer with transrectal ultrasound-guided biopsy, no relationship was observed between serum testosterone level and prostate cancer severity. [SUP][43][/SUP] Thus, it is possible that the relationship between testosterone level and Gleason score is indeed most significant in older men with more aggressive tumors.
Our study was limited by several factors. First, the study was performed with a cohort of men diagnosed with prostate cancer. Although the considerations for questionnaire score are addressed above, it is also possible that unaccounted for factors, including individual differences in anxiety levels before major surgery or as a result of the cancer diagnosis, may have affected both IGF-1 levels and erectile function. Second, most of the correlations, save for those in the >70-year-old age group, are fairly low. Although this could be a result of the factors above, there may be additional variables that affect the relationship between the GH axis and sexual function and are currently unaccounted for.
Considering the overlap between GH and testosterone in the pathogenesis of erectile dysfunction, it may be beneficial to evaluate both the testosterone and GH axes when evaluating etiology and considering the treatment of erectile dysfunction. Our results support a relationship between IGF-1 and male sexual function, and strengthen the argument to more closely study the role of IGF-1 in erectile dysfunction. There do not exist sufficient data to use IGF-1 or GH supplementation in men with erectile dysfunction currently, and studies demonstrating a role of GH and IGF-1 in development and progression of prostate cancer may further temper this possibility. However, recent studies, including ours, show potential and promise for new ways to enhance current treatment protocols that could improve quality of life in men with erectile dysfunction.
References
- Erfurth EM, Hagmar LE, Saaf M, Hall K. Serum levels of insulin-like growth factor I and insulin-like growth factor-binding protein 1 correlate with serum free testosterone and sex hormone binding globulin levels in healthy young and middle-aged men. Clin Endocrinol (Oxf) 1996; 44: 659–664.
- Muniyappa R, Sorkin JD, Veldhuis JD, Harman SM, Munzer T, Bhasin S et al. Long-term testosterone supplementation augments overnight growth hormone secretion in healthy older men. Am J Physiol Endocrinol Metab 2007; 293: E769–E775.
- Wang C, Nieschlag E, Swerdloff R, Behre HM, Hellstrom WJ, Gooren LJ et al. ISA, ISSAM, EAU, EAA and ASA recommendations: investigation, treatment and monitoring of late-onset hypogonadism in males. Int J Impot Res 2009; 21: 1–8.
- Araujo AB, Esche GR, Kupelian V, O'Donnell AB, Travison TG, Williams RE et al. Prevalence of symptomatic androgen deficiency in men. J Clin Endocrinol Metab 2007; 92: 4241–4247.
- Bain J. Andropause. Testosterone replacement therapy for aging men. Can Fam Physician 2001; 47: 91–97.
- Vermeulen A. The future of hormone replacement therapy in the aging male. Aging Male 2000; 3: 210–213.
- Foresta C, Zuccarello D, De Toni L, Garolla A, Caretta N, Ferlin A. Androgens stimulate endothelial progenitor cells through an androgen receptor-mediated pathway. Clin Endocrinol (Oxf) 2008; 68: 284–289.
- Malkin CJ, Pugh PJ, Morris PD, Kerry KE, Jones RD, Jones TH et al. Testosterone replacement in hypogonadal men with angina improves ischaemic threshold and quality of life. Heart 2004; 90: 871–876.
- Navarro-Dorado J, Orensanz LM, Recio P, Bustamante S, Benedito S, Martinez AC et al. Mechanisms involved in testosterone-induced vasodilatation in pig prostatic small arteries. Life Sci 2008; 83: 569–573.
- Seyrek M, Yildiz O, Ulusoy HB, Yildirim V. Testosterone relaxes isolated human radial artery by potassium channel opening action. J Pharmacol Sci 2007; 103: 309–316.
- Kouloumenta V, Hatziefthimiou A, Paraskeva E, Gourgoulianis K, Molyvdas PA. Non-genomic effect of testosterone on airway smooth muscle. Br J Pharmacol 2006; 149: 1083–1091.
- Dominguez JM, Gil M, Hull EM. Preoptic glutamate facilitates male sexual behavior. J Neurosci 2006; 26: 1699–1703.
- Motofei IG. A dual physiological character for sexual function: libido and sexual pheromones. BJU Int 2009; 104: 1702–1708.
- Corpas E, Harman SM, Blackman MR. Human growth hormone and human aging. Endocr Rev 1993; 14: 20–39.
- Kaufman JM, Taelman P, Vermeulen A, Vandeweghe M. Bone mineral status in growth hormone-deficient males with isolated and multiple pituitary deficiencies of childhood onset. J Clin Endocrinol Metab 1992; 74: 118–123.
- Juul A, Scheike T, Davidsen M, Gyllenborg J, Jorgensen T. Low serum insulin-like growth factor I is associated with increased risk of ischemic heart disease: a population-based case-control study. Circulation 2002; 106: 939–944.
- Laughlin GA, Barrett-Connor E, Criqui MH, Kritz-Silverstein D. The prospective association of serum insulin-like growth factor I (IGF-I) and IGF-binding protein-1 levels with all cause and cardiovascular disease mortality in older adults: the Rancho Bernardo Study. J Clin Endocrinol Metab 2004; 89: 114–120.
- McCallum RW, Petrie JR, Dominiczak AF, Connell JM. Growth hormone deficiency and vascular risk. Clin Endocrinol (Oxf) 2002; 57: 11–24.
- Uckert S, Scheller F, Stief CG, Knapp WH, Sohn M, Becker AJ et al. Potential mechanism of action of human growth hormone on isolated human penile erectile tissue. Urology 2010; 75: 968–973.
- Becker AJ, Uckert S, Stief CG, Truss MC, Machtens S, Scheller F et al. Possible role of human growth hormone in penile erection. J Urol 2000; 164: 2138–2142.
- Wang C, Nieschlag E, Swerdloff R, Behre HM, Hellstrom WJ, Gooren LJ et al. Investigation, treatment and monitoring of late-onset hypogonadism in males. Int J Androl 2009; 32: 1–10.
- Burnett AL, Lowenstein CJ, Bredt DS, Chang TS, Snyder SH. Nitric oxide: a physiologic mediator of penile erection. Science 1992; 257: 401–403.
- Jung GW, Kwak JY, Yoon S, Yoon JH, Lue TF. IGF-I and TGF-beta2 have a key role on regeneration of nitric oxide synthase (NOS)-containing nerves after cavernous neurotomy in rats. Int J Impot Res 1999; 11: 247–259.
- Pu XY, Wang XH, Gao WC, Yang ZH, Li SL, Wang HP et al. Insulin-like growth factor-1 restores erectile function in aged rats: modulation the integrity of smooth muscle and nitric oxide-cyclic guanosine monophosphate signaling activity. J Sex Med 2008; 5: 1345–1354.
- Guler HP, Zapf J, Schmid C, Froesch ER. Insulin-like growth factors I and II in healthy man. Estimations of half-lives and production rates. Acta Endocrinol (Copenh) 1989; 121: 753–758.
- Keenan BS, Richards GE, Ponder SW, Dallas JS, Nagamani M, Smith ER. Androgen-stimulated pubertal growth: the effects of testosterone and dihydrotestosterone on growth hormone and insulin-like growth factor-I in the treatment of short stature and delayed puberty. J Clin Endocrinol Metab 1993; 76: 996–1001.
- Thum T, Hoeber S, Froese S, Klink I, Stichtenoth DO, Galuppo P et al. Age-dependent impairment of endothelial progenitor cells is corrected by growth-hormone-mediated increase of insulin-like growth-factor-1. Circ Res 2007; 100: 434–443.
- Mulhall JP. Exploring the potential role of neuromodulatory drugs in radical prostatectomy patients. J Androl 2009; 30: 377–383.
- Becker AJ, Uckert S, Stief CG, Scheller F, Knapp WH, Hartmann U et al. Serum levels of human growth hormone during different penile conditions in the cavernous and systemic blood of healthy men and patients with erectile dysfunction. Urology 2002; 59: 609–614.
- Cappelleri JC, Althof SE, Siegel RL, Stecher VJ, Tseng LJ, Duttagupta S. Association between the Erectile Dysfunction Inventory of Treatment Satisfaction and the Self-Esteem and Relationship Questionnaire following treatment with sildenafil citrate for men with erectile dysfunction. Value Health 2005; 8(Suppl 1): S54–S60.
- Wei JT, Dunn RL, Litwin MS, Sandler HM, Sanda MG. Development and validation of the expanded prostate cancer index composite (EPIC) for comprehensive assessment of health-related quality of life in men with prostate cancer. Urology 2000; 56: 899–905.
- Rhoden EL, Teloken C, Sogari PR, Souto CA. The relationship of serum testosterone to erectile function in normal aging men. J Urol 2002; 167: 1745–1748.
- Yassin AA, Saad F. Improvement of sexual function in men with late-onset hypogonadism treated with testosterone only. J Sex Med 2007; 4: 497–501.
- Rhoden EL, Morgentaler A. Symptomatic response rates to testosterone therapy and the likelihood of completing 12 months of therapy in clinical practice. J Sex Med 2010; 7(1 Part 1): 277–283.
- Chiang HS, Cho SL, Lin YC, Hwang TI. Testosterone gel monotherapy improves sexual function of hypogonadal men mainly through restoring erection: evaluation by IIEF score. Urology 2009; 73: 762–766.
- Higashi Y, Sukhanov S, Anwar A, Shai SY, Delafontaine P. IGF-1, oxidative stress and atheroprotection. Trends Endocrinol Metab 2010; 21: 245–254.
- D'Ercole AJ, Stiles AD, Underwood LE. Tissue concentrations of somatomedin C: further evidence for multiple sites of synthesis and paracrine or autocrine mechanisms of action. Proc Natl Acad Sci USA 1984; 81: 935–939.
- Chopin LK, Veveris-Lowe TL, Philipps AF, Herington AC. Co-expression of GH and GHR isoforms in prostate cancer cell lines. Growth Horm IGF Res 2002; 12: 126–136.
- Rowlands MA, Gunnell D, Harris R, Vatten LJ, Holly JM, Martin RM. Circulating insulin-like growth factor peptides and prostate cancer risk: a systematic review and meta-analysis. Int J Cancer 2009; 124: 2416–2429.
- Mucci LA, Stark JR, Pollak MN, Li H, Kurth T, Stampfer MJ et al. Plasma levels of acid-labile subunit, free insulin-like growth factor-I, and prostate cancer risk: a prospective study. Cancer Epidemiol Biomarkers Prev 2010; 19: 484–491.
- Gill JK, Wilkens LR, Pollak MN, Stanczyk FZ, Kolonel LN. Androgens, growth factors, and risk of prostate cancer: the Multiethnic Cohort. Prostate 2010; 70: 906–915.
- Pierorazio PM, Ferrucci L, Kettermann A, Longo DL, Metter EJ, Carter HB. Serum testosterone is associated with aggressive prostate cancer in older men: results from the Baltimore Longitudinal Study of Aging. BJU Int 2010; 105: 824–829.
- Morote J, Ramirez C, Gomez E, Planas J, Raventos CX, de Torres IM et al. The relationship between total and free serum testosterone and the risk of prostate cancer and tumour aggressiveness. BJU Int 2009; 104: 486–489.
<!-- article content ends here -->
")