Year: 2019
Does Trenbolone Cause Alzheimer’s Disease? | What The Data Shows
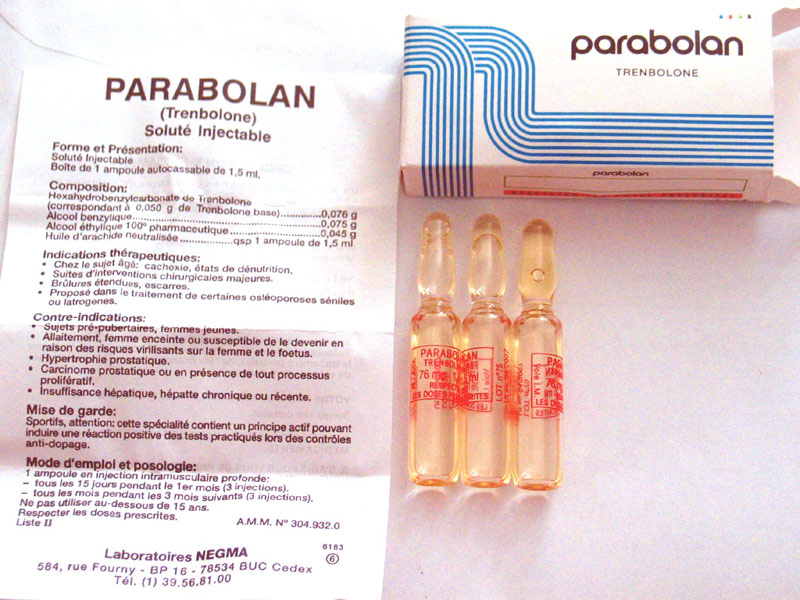
After clinical data started circulating in the bodybuilding community showing that Trenbolone administration caused beta amyloid plaque accumulation in rat brains, more and more attention has been given to the potential neurodegenerative effects it may have in humans, and how Trenbolone may cause the progression of Alzheimer’s disease.Without even delving into the clinical data, most will agree that Trenbolone blatantly exhibits some worrisome effects on cognitive health.If you’ve used it, I’m sure you can attest to the fact that no other steroid is on par when it comes to the effects it seems to have on the mind.The fact is, it is one of the most volatile steroids for cognitive health and mental state.Some guys can’t even use it because it gives them such bad mental side effects.[embedded content]Table of ContentsThe Effect Trenbolone Has On Your MindTrenbolone is jokingly (but also fairly accurately) called the “relationship destroyer” drug.Aggression and volatility of your mood can occur with any androgen, and the degree to which this happens is largely dependent on the androgenicity of the steroid in question.If you have an aggressive personality, increasing your body’s androgen load is going to exacerbate that.Trenbolone in particular though seems to have a bit of a different effect that is not found with any other compound.Some guys feel great, but many feel extremely anxious, paranoid, have volatile mood swings, and are much more easily agitated when compared to how they feel using other anabolic-androgenic steroids.I don’t think it’s a coincidence that the rats that had Trenbolone administered to them in the clinical studies experienced significant neurodegeneration.The Trenbolone Dosage Protocol In Humans Via Negma Laboratories (Parabolan)The dose is the poison when it comes to steroids, and Trenbolone is no different.The first thing to take into consideration when it comes to the neurodegenerative impact Trenbolone has on humans is the dosage deployed for bodybuilding purposes.Trenbolone abuse is rampant in the fitness industry nowadays, and teenagers on their first steroid cycle are using Trenbolone dosages higher than what farmers use to beef up cattle.[embedded content]Trenbolone has no place in a first cycle, nor does it have a place in any cycle except for a couple token scenarios in my opinion.Pharmaceutical grade Trenbolone used to be produced for human use by Negma Laboratories under the brand name Parabolan, but there were no published human trials.It was pulled from the market in 1997 and is no longer approved for human use.The Trenbolone dosage used in a clinical setting for humans was purportedly three 76 mg Parabolan ampules per month.This equates to approximately 50 mg of active hormone per ampule after cleaving off the ester.This had a front load period of three Parabolan ampules over the first 15 days, followed by a maintenance phase of one Parabolan ampule every 10 days thereafter.114 mg Trenbolone Hexahydrobenzylcarbonate (75 mg active hormone) per week for the first two weeks76 mg Trenbolone Hexahydrobenzylcarbonate (50 mg active hormone) per 10 days thereafterIFBB Pro bodybuilders in the 90’s had success with Trenbolone following similar dosage protocols.Does that mean that those dosages were safe?No, not at all.But, there is a dose dependent increase in risk with this compound, and the dosages unnecessarily being used nowadays are insane to say the least.Based on the clinical data, we can see a dose dependent accumulation of beta amyloid plaque in the brains of the rodents administered Trenbolone, which more than likely has significant crossover into humans.Trenbolone Contributes To NeurodegenerationThe study that drew the most attention to Trenbolone’s effect on neurodegeneration is titled: “17β-trenbolone, an anabolic-androgenic steroid as well as an environmental hormone, contributes to neurodegeneration [R].”This part of the study is the most notable: “Trenbolone accumulated in adult rat brain, especially in the hippocampus and in the fetus brain, it altered amyloid-beta-42 accumulation. Trenbolone induced apoptosis of primary hippocampus neurons in vitro and resisted neuroprotective function of testosterone.”Apoptosis is cell death.Trenbolone not only caused cell death of neurons in the brain, but it caused amyloid-beta-42 to accumulate in a dose dependent manner.Trenbolone Causes Beta Amyloid Plaque AccumulationThe male rats given Trenbolone injections had amyloid-beta-42 (also referred to as beta amyloid) accumulate in their brains.Alzheimer’s disease is believed to be caused by the accumulation of the beta amyloid peptide.While there has been no human trial to assess if this occurs in humans, and there probably is never going to be, I think it is best to assume the worst when we see data like this.As I already touched on, I do not think it is a coincidence that guys get very strange mental side effects from Tren that they don’t get with other compounds.Beta amyloid plaque build up doesn’t just occur with Trenbolone use obviously, and our body does have internal mechanisms in place to clean the brain of it each day.Healthy individuals clear beta amyloid out of the brain during deep sleep via glymphatic drainage.Basically, beta amyloid builds up and then the brain cleans it up during deep sleep.If sleep quality and/or duration is impaired, expectedly, drainage via the glymphatic system is impaired too, and beta amyloid plaque then starts to accumulate over time, which can eventually cause Alzheimer’s disease and a myriad of other neurodegenerative outcomes.This is why so many neurodegenerative diseases have been linked to poor sleep quality.If you don’t have enough “brain cleaning” occurring each night because of poor sleep, you will eventually pay the toll in some way with impaired cognitive function.While this is a rodent model, if you’re injecting something that has shown to increase the literal compound in your brain proven to be the root of Alzheimer’s disease in a dose dependent manner, you can surmise that this probably isn’t the best compound to be using on a consistent basis.Should You Ever Use Trenbolone Based On The Neurotoxicity Data?Remember, the dose is the poison with any drug.While Trenbolone isn’t safe and will be more neurotoxic and cardiotoxic the higher the dosage deployed, you can’t argue with the fact that it is an amazing drug for body composition.I believe Trenbolone has a place in a competitive bodybuilder’s toolbox pre-contest.Trenbolone has shown to be more protein sparing than other steroids, and is why it shines so much in a calorie deficit during a contest prep phase [R].When it comes to protein accretion though (muscle building), Trenbolone does not outperform other compounds that have significant amounts of human-based safety, efficacy and tolerability data for us to reference.There are other hormones just as effective at building lean muscle mass, without as much potential risk associated with screwing up your brain.Considering this, the only time short-term use of Trenbolone makes sense is during the last couple months of a contest prep.There are a lot of guys using Trenbolone during every single cycle, which is overkill.Although purely anecdotal, I’ve personally seen guys who cruise on Tren year round progressively act more and more “off” each time I saw them.Its almost like you can just tell there is a screw loose that wasn’t loose before with guys who abuse Tren.Using Trenbolone short-term pre-contest is a calculated risk, and I would advise limiting its use, or avoiding it entirely if you can.The Vicious Circle Of Deep Sleep, Beta Amyloid Plaque And Alzheimer’s ProgressionDr. Matthew Walker is a scientist and professor of neuroscience and psychology at the University of California.His research focuses on the impact of sleep on human health and disease.In the following clip he describes the role that sleep plays in modulating the accumulation of amyloid-beta accumulation in the brain.I highly recommend that you watch the entire thing, or read through the transcription I wrote out below, as it elucidates exactly how sleep impacts cognitive health and neurodegenerative outcomes, and also provides insight into exactly how Trenbolone abuse will likely encourage the progression of Alzheimer’s disease and neurodegeneration.At the end of the article I tie together Matthew Walker’s points outlined in the clip and relate it back to how it applies to Trenbolone use, as well as how to track metrics that will help you assess your cognitive health and sleep quality.[embedded content]“Of those electrical deep brain waves of deep sleep.It seems as though they come from all over the brain.But the principal epicenter that generates your deep sleep sits right there in the middle part of the prefrontal cortex.It is exactly the same part of the brain that accumulates toxic beta amyloid protein.Then, we’ve done studies, and other people have done studies before us, that have demonstrated as we age, our sleep gets worse.But not just any type of sleep, especially that deep quality of sleep that we know and we spoke about is critical for saving, learning, and retaining new memories.All of these jigsaw pieces started to get put together.In my head, I thought we need to do some studies.Is it possible that the amount of amyloid that you have in the brain in this sleep-generating center, it should directly predict the deficit in the amount of deep sleep that you get?If it predicts the deficit in the amount of deep sleep, it should predict the deficit in your ability to hold on and retain new memories, which is a hallmark cognitive feature of Alzheimer’s disease: difficulty learning, difficulty retaining.We did the study, and that’s exactly what we found: the more beta amyloid that builds up in this central frontal part of the brain, the less the deep sleep that you have; the less amyloid-related deep sleep that you had, the more forgetful you were the next day, rather than the more that you remembered.This was the first part of the Alzheimer’s sleep equation, which is that Alzheimer’s disease attacks the deep sleep-generating regions, and you have a diminution of deep sleep, which, in turn, blunts your learning and memory abilities, and you become more forgetful.A far more important discovery was made by another group, far more important than the one we made, which was essentially the reverse direction.Which was to say, rather than amyloid sort of decreasing sleep, could sleep actually decrease the amount of amyloid that you get.This was a discovery that was made in rats back in 2009.I believe it was the first evidence that was published in science.This is a colleague, Dr. Neta Garden, who is out on the East Coast at University of Rochester.She made two wonderful discoveries.The first, was that we’ve known for a long time the body has a waste sewage system called the lymphatic system.But the brain doesn’t have its own lymphatic system: the lymphatic system does not penetrate the brain.Where does all of the garbage, the metabolic garbage, go that your brain cells produce?Where’s the sewage system for the brain?She discovered it.It’s actually made up of a set of cells called glial cells, which are the supporting brain cells.So, she called it the “glymphatic system” rather than the lymphatic system.Your brain does have a sewage system: this glymphatic system.That’s the discovery that she made.Remarkable!Then, and I’m not quite sure what motivated her to do this, she started to measure how efficient that lymphatic waste system was.When the rats were awake and when the rats were asleep?What she found was that it’s during deep sleep, that these brain cells actually shrink by almost 60%.When we sleep, blows my mind, it’s almost like all of the buildings in New York all of a sudden shrink, and it leaves these much greater large areas for the cleaning crews to come in and clean up all of the metabolic detritus of the city’s activity during the day.That’s exactly what happens during sleep.The cleaning solution is what we call cerebrospinal fluid.Through a pulsatile mechanism during sleep, you get a 10 to 20% increase in the bathing of cerebrospinal fluid through the brain, which washes away all of the metabolic byproducts that have been building up.One of those metabolic byproducts is beta amyloid.In fact, if you deprive those rats of that deep sleep, you immediately get an increase in toxic beta amyloid.Now, we’ve linked these terms, right?It’s a long story.But if you’re not getting enough deep sleep at night, you’re not giving yourself the chance for the kind of good “night-and-sleep clean process” to remove the beta amyloid, so more beta amyloid builds up.Where does it build up?Tragically, in the very same regions of the brain that generate the deep sleep that you need to clear out the toxic amyloid.So, you start getting less deep sleep, so you get more toxic protein; more toxic protein, less deep sleep, less deep sleep.It’s a self-fulfilling prophecy.It’s a nonlinear exponential curve.If you look at how amyloid builds up in the brain, and if you look at the trajectory of Alzheimer’s disease, it is a nonlinear exponential curve.It fits exactly what the sleep-dependent model of amyloid-clearance would predict, if you’re not getting sufficient sleep.That’s the reason why now insufficient sleep seems to be one of the most significant lifestyle factors determining that.Now, you could say, by the way, those studies were in rats, and you deprive them of sleep for one night, what about humans, like, surely?Well, the study is now being done.Great study done out of “Wash U” by a team of scientists, led by David Holtzman.They took a group of humans and they did this very clever method where they deprive them of deep sleep, but they didn’t deprive them of sleep.You think that sounds paradoxical.I can play you these auditory tones.Now, this is not like the memory reactivation word that you play a tone and then you leave the brain alone for a while.Here, I’m just going to keep playing tones to your brain, really sort of annoying tones.I can play them at a level that doesn’t wake you up, but it lifts you out of deep sleep and keeps you in shallow sleep.What’s delightful about this method is that I can selectively excise one type of sleep, deep sleep, but I don’t wake you up.There’s no stress of awakening.You are asleep for the same amount of time, but the quality of sleep is decreased.Can street noise do that?We don’t know.Although, I will come back to that when we speak about, hopefully sleep, appetite regulation, sleep glucose regulation, and sleep in low socio-economic.I think it’s possible there’s other factors that link poor sleep in low SES socioeconomic backgrounds.Is noise pollution one of them?I actually think it is.Untested, as yet.But what they did with these human participants, they selectively removed deep sleep while keeping them asleep.Total sleep time has not changed.Then, in the morning, they woke them up, they rolled them over, and they did a spinal cord puncture, lumbar puncture, and they measured the cerebral spinal fluid that was percolating within the spinal cord which also goes around the brain.You can measure the amount of beta amyloid, which is a reflection of perhaps how much amyloid is there within the brain.After one night of essentially a loss of deep sleep, you saw an immediate rise in the amount of beta amyloid.It is a causal manipulation, that insufficient sleep in rodents and in humans, will lead to a rise in beta amyloid.I think it was like 25 to 30%.It was.It was.Yeah.”Trensomnia And How Trenbolone Can Potentially Cause Alzheimer’s DiseaseAs Matthew outlined in the clip above, the area of the brain that beta amyloid plaque builds up in is the same area of the brain responsible for getting into the stage of deep sleep required for cleaning beta amyloid out of your brain.What I found most interesting about this is the fact that in humans, one of the main side effects of Tren most commonly reported that is unique to that compound is something called “Trensomnia.”Trensomnia is the insomnia and poor quality sleep that many get when using Trenbolone.Trenbolone is notorious for ruining sleep quality, and that is just one of the attributes of Trenbolone that make it unique from other steroids.I think that in itself makes it pretty clear what mechanism is likely occurring with Trenbolone use not just in rodents, but in humans as well.Trenbolone use inhibits deep sleep severely, which in turn results in impaired beta amyloid clean up via the glymphatic system, consequently increasing the amount of beta amyloid plaque accumulation in the brain, which ultimately results in neurodegeneration.The more beta amyloid that builds up, the worse the quality of sleep becomes, and the worse the quality of sleep becomes, the more beta amyloid plaque will accumulate.This is the vicious circle Trenbolone can have on the brain, at least in theory.Is Trenbolone going to cause Alzheimer’s disease?I don’t know.But it seems pretty damn convincing that Trenbolone abuse will at least result in some level of neurodegeneration based on this correlation here, as well as what we see all the time anecdotally in humans who abuse this compound.If you’ve used Trenbolone before, you can likely personally attest to how significant of an impact it has on your sleep quality.Imagine what Trenbolone is doing to the brains of men using it year round.Are you ever actually getting enough deep sleep to clean up beta amyloid accumulated in the brain when you’re on Trenbolone?If you’re abusing Trenbolone you are probably more likely to get cardiovascular disease before you get full blown Alzheimer’s, but that does not mean that you should abuse it based on the fact that neurodegeneration is a slow and long-term process.How To Track Your Sleep QualityA very interesting experiment would be to assess Oura ring metrics before and during Trenbolone use.I use an Oura ring every single night to track my sleep metrics. The Oura ring will give you metrics as accurate as you’re going to get without literally going in and getting an elaborate and expensive sleep study done with medical-grade equipment.The ring will estimate with a fairly high level of accuracy how much sleep you’re getting per night, your REM sleep, deep sleep, resting heart rate, heart rate variability, body temperature, among several other useful metrics.If you’re an anabolic steroid user and you have established average baseline metrics of your sleep quality with the Oura ring and then you introduce Trenbolone into your protocol and suddenly your metrics show that your deep sleep has been severely impaired, I believe that would be more than convincing for me to make an assertion that Trenbolone will dramatically increase your chance of getting Alzheimer’s disease.Related
NPC Nationals Mens Classic Physique and Womens Physique Backstage Video
NPC Nationals Mens Classic Physique and Womens Physique Backstage Video NATIONAL PHYSIQUE COMMITTEE RULE CHANGE: GREEN CARDS November 26, 2019 At the NPC National Board Of Governor’s Meeting held at the 2019 NPC National Championships, a New Rule was enacted in regard ALL United States Valid Green Card Holders. Starting in 2020, All…
How To Break Through A Plateau On A Steroid Cycle | Logical Steroid Use Practices
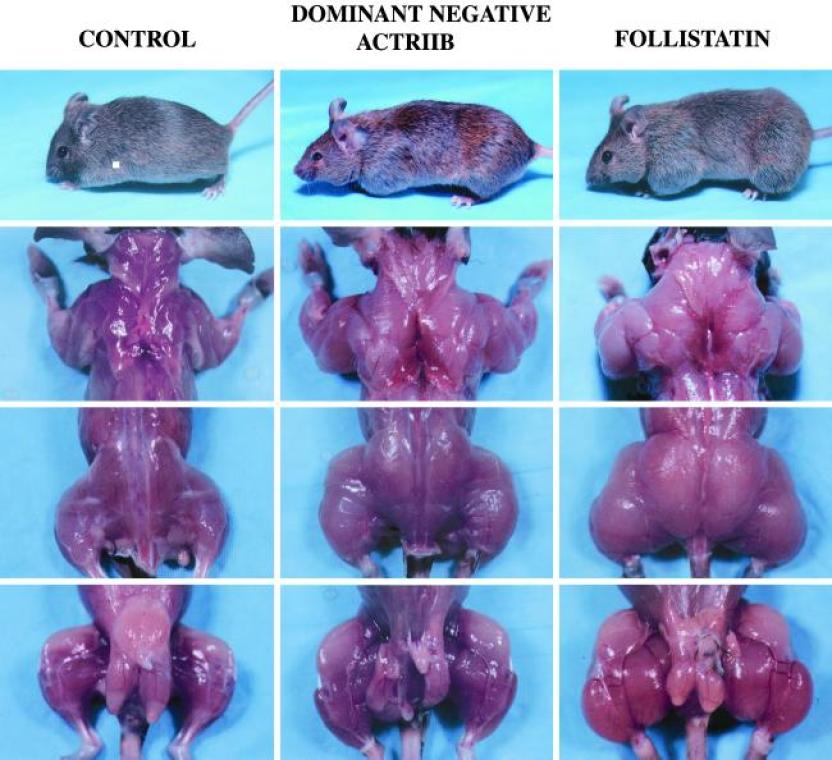
When I first started getting into bodybuilding and learning about pharmacology, a strategy I would see commonly advised on forums and by industry gurus was switching compounds at week 6 or week 8 to avoid androgen receptor downregulation and circumvent a plateau on a steroid cycle.This strategy is still used just as commonly today.Basically, the hypothesis was that you should be switching steroids every 6-8 weeks, or else your body gets used to them and they will stop working.At the time, this made complete sense to me.Logically you would think that if you use a steroid your body will eventually get used to it and then you will have to switch steroids to keep your body guessing.Almost like muscle confusion.An example of a “good” bulking cycle based on this widespread belief will commonly look something like this:Testosterone EnanthateNandrolone DecanoateTrenbolone EnanthateWeek 1-8500 mg400 mgWeek 1-16500 mg 400 mgAt week 8, according to bro-science, your body is now too used to the Deca and switching compounds to something like Trenbolone is necessary to continue growing at the same pace.Besides the fact that the Deca is actually going to be in your system anyways occupying androgen receptors for months past the point of switching compounds, objectively to many newbies learning about this stuff for the first time, this cycle might look good.[embedded content]Over the years as I’ve done more research, I’ve started to realize how ridiculous this bro science switching compounds theory is.It actually gets under my skin that somebody didn’t publicly come out with the truth dispelling this myth sooner, as it would have prevented me from using compounds with far less favorable side effect profiles that I didn’t even need to use to achieve my goals.Table of ContentsAll Steroids Basically Do The Same ThingAndrogen receptor activation is accomplished via the same mechanism of action by any steroid (more or less).Steroids bind to the androgen receptor and transcribe anabolic and androgenic effects in tissues in the body.Interestingly enough, the human body generally responds in almost the same way to any anabolic steroid, as they all more or less do the same thing at the end of the day.“After 1935 the best method of discovering and measuring the protein-building action of androgenic steroids in humans proved to be metabolic balance studies. In 1955, when anabolic steroids with less androgens were developed, the nitrogen-balance method was used again to evaluate and compare the nitrogen-sparing effect of the various preparations. The findings of the numerous balance studies that were performed are as follows: The injectable 17 beta-esters, such as nandrolone phenylpropionate, nandrolone decanoate and methenolone enanthate exert a strong anabolic action for several weeks, amounting to 2-2.50 g nitrogen/day, which corresponds to a daily gain of 12-15 g protein or 60-75 g lean body mass. The orally active 17-alkyl derivatives induce a dose-dependent nitrogen-saving effect of the same order.”Nitrogen retention and protein accretion were roughly the same between all of the steroids evaluated in the study above, which are all compounds commonly switched in and out of cycles nowadays [R].Some steroids are more tissue selective, some will antagonize SHBG and/or Estrogen more than others, some will result in a dryer cosmetic look that differs from another, but when it comes to lean muscle growth, they all more or less do the same thing in a nitrogen retention context.Considering this, it would be wise to choose the most well tolerated anabolic agents with the lowest risk profile you can to accomplish your bodybuilding goals.If nitrogen sparing is more or less the same between two compounds, but one has far less clinical data backing its safety profile and tolerability, why is it that so many guys are reaching for the highest risk compounds they can whenever given the opportunity?It is not uncommon nowadays to see bros reach for something like DHB (Dihydroboldenone) instead of Nandrolone because of the exotic appeal, and they heard a couple bros on the forums say that it is “like Tren without the side effects.”Use something with zero data on humans and had sh*t results in the one preclinical rodent model published on it, or use something with lots of clinical data that has proven for years to be one of the most well tolerated mass building agents we can deploy?I’m sure you can figure out what the logical choice is here.Androgen Receptors Upregulate In the Presence Of Androgens, Not DownregulateSwitching compounds at week 8 is done to avoid a potential plateau on a steroid cycle by circumventing the supposed androgen receptor downregulation that occurs after a couple months on the same steroid.The fact is that the complete opposite occurs.Androgen receptors upregulate in the presence of androgens, not downregulate.[embedded content]Androgens facilitate their anabolic effects in tissues through their action on multiple cellular targets.Testosterone increases satellite cell replication and activation, the number of myonuclei, and increases protein accretion.The myogenic effects on cellular differentiation, proliferation, and muscle protein turnover are accomplished through multiple signaling pathways via the androgen receptor.Androgen receptors, in the satellite cell as well as several other muscle cell types, are upregulated by androgens [R, R].We’ve known this since the 80’s [R].If androgen receptors don’t downregulate with steroid use, then what is causing muscle growth to slow down and plateau?The main factor that appears to play a role in muscle growth inhibition is the elevation of a protein in the body called Myostatin.How Myostatin Inhibits Muscle GrowthMyostatin is a protein in the body that acts as a regulator of skeletal muscle mass, limiting how much muscle the body can grow [R].Examples of Myostatin deficiencies are found in lab based rodent models, as well as in the farming industry with Myostatin deficient cattle.Myostatin Knockout MiceMice that lack the gene that creates Myostatin have approximately twice as much muscle mass as normal mice [R].Belgian Blue Double-Muscled CattleThe Belgian Blue has a Myostatin gene mutation, consequently preventing its feedback loop of muscle growth inhibition from working correctly.This mutation interferes with fat deposition and can lead to accelerated lean muscle growth.The acceleration of muscle growth in Belgian Blues is due primarily to physiological changes in the animal’s muscle cells (fibers) from hypertrophy to a hyperplasia mode of growth.This growth occurs in the fetus and results in a calf being born with two times the number of muscle fibers as a calf without a Myostatin gene mutation [R].Myostatin Elevates In Response To AndrogensWhile there are likely other counterregulatory mechanisms in the body that inhibit excessive muscle growth, the main factor appears to be Myostatin elevation.Your body doesn’t experience androgen receptor downregulation by week 8 that would then make switching compounds necessary, rather, Myostatin elevates in response to supraphysiological amounts of exogenous androgens and inhibits muscle growth, regardless of what compound is being used.Switching from NPP to EQ at week 8 will change absolutely nothing when it comes to androgen receptor sensitivity and breaking a plateau.Myostatin increases to prevent you from gaining unhealthy amounts of muscle.When you take your Testosterone replacement therapy and your Testosterone binds to androgen receptors, do you eventually have to increase your dose of Testosterone or cycle off of Testosterone to make your TRT work again?Of course not.Just like you don’t need to cycle off of your own balls producing Testosterone, because they bind to the androgen receptor in exactly the same way and do not downregulate it.The only thing that downregulates is your ability to accrue muscle mass in response to androgen receptor activation because of the elevation of inhibiting mechanisms in your body, namely Myostatin.When you hit week 8 of a cycle and Myostatin is elevated because of your use of supraphysiological amounts of androgens, your body is trying to prevent you from gaining an unhealthy amount of muscle.This is why you plateau on a cycle, not because the steroid you are using just stops working.In the following study, the effects of exogenous Testosterone and Trenbolone on Myostatin levels was evaluated [R].This study showed that after 29 days of administration of either Testosterone or Trenbolone, Myostatin protein levels were 197% higher in the castrated and Testosterone group, and 209% higher in the castrated and Trenbolone group when compared to the placebo.There’s a reason why this mechanism is in place in our bodies and we can’t grow linearly.Too much of anything is not going to be good, and when you try to push your body to a place that isn’t healthy, homeostatic mechanisms in the body will try to stop you.The human body is a big balancing act.More Androgens = More Myostatin = More Muscle Growth InhibitionAs previously outlined, Myostatin is a growth inhibitor that elevates in the presence of androgens.Based on the current research it appears that the higher your dose of exogenous anabolics, the greater muscle growth potential you have, and consequently the higher your Myostatin will elevate in parallel to inhibit absurd rates of muscle growth.In a study evaluating the effect graded doses of Testosterone have on Myostatin levels in young and older men, Myostatin levels were significantly higher on day 56 than baseline in both groups [R].The Myostatin hypothesis isn’t air tight and has some holes in the data contradicting its muscle growth inhibiting effects.However, based on what we know to date, the research suggests that its more than likely the main regulatory mechanism involved in muscle growth response relative to androgen receptor activation.Myostatin is well known to negatively regulate muscle mass in mice, cattle, dogs and humans [R].Why Switching Compounds To Deal With “Downregulation” Is A Bad IdeaSwitching compounds to break through your plateau will make no difference on your outcomes.At the end of the day, Myostatin will elevate relative to the anabolic stimulus in the body.Increase your Testosterone more, Myostatin will elevate.Switch from Primobolan to Masteron at week 8 and what will happen?Nothing, androgen receptors are already upregulated and sensitive enough to do what they are supposed to do, but Myostatin will remain elevated regardless of what compounds you switch in and out.If you experience a plateau on a cycle, switching steroids doesn’t circumvent the root of the issue.If you switch to something stronger, then Myostatin will only increase even more to match this increase in androgen load in the body.Switching from Nandrolone to Tren, to EQ, and just randomly swapping things in and out has no effect on transcription at the androgen receptor, the only thing that will change is your body’s production of Myostatin relative to your doses and muscle growth potential (and potentially other undiscovered counterregulatory factors as well).The main problem with switching compounds in this manner is that you could be using a thoroughly studied compound with very good clinical outcomes, high tolerability in humans, and a very favorable safety profile (e.g. Testosterone, Nandrolone, or Primobolan), and then end up switching to a compound with a far less favorable safety profile riddled with side effects just to achieve the same rate of muscle growth you already had achieved with the safer option.Bodybuilding gurus will tell their clients to switch from Deca to Trenbolone at week 8 in the offseason simply because of this androgen receptor downregulation broscience, and then put their client in a terrible position where they are using a far more risky compound to achieve nearly the same level of nitrogen retention in the body.I can’t even fathom how many times this has happened now where a bodybuilder will be using thoroughly studied compounds with hordes of clinical data on humans and switch to some obscure, high-risk steroid with nearly identical muscle growth potential based solely on this androgen receptor hypothesis.I vividly remember all the bulk phases I did in the past where I would hit week 8 and then wonder what I should do.If you’re using Nandrolone and you get to week 8, what do you swap to?Switch to another 19-nor?Trestolone?Or am I going switch to Tren during the offseason because my Nandrolone has “stopped working” at week 8?This is the kind of information that hordes of clueless coaches are pushing on their clients.You could be on a strong foundation of androgens with a great efficacy profile and then have your cookie cutter guru come out and tell you that you need to switch to a compound that’s more dangerous and no better at building muscle than what you’re using because the compounds you’re using are “no longer working,” when it just isn’t the case whatsoever.Remember, these compounds all more or less do the same thing, so doesn’t it make sense to choose the compounds that build the most muscle with the least side effects, and to stick with those as your staples?Certain compounds that produce a unique cosmetic look of the muscle should be reserved for pre-contest use only in my opinion, as muscle growth can be achieved during a mass building phase with less risky options.What To Do After You Plateau On A Steroid Cycle And Myostatin Is ElevatedOnce you get deep enough into a cycle, you will plateau.Now that we have established that the proper course of action IS NOT switching compounds to overcome this nonexistent androgen receptor downregulation, what exactly can you do?You have a few options here.Increase Your Calorie IntakeThis should be the first thing you do.Every time you plateau, try increasing your calorie intake a tad.As little as an additional 100-200 calories per day can be enough to get you gaining again.Do this until you plateau in strength and size gains and the subsequent increase in your calorie intake just results in more body fat gain.Increase Your DoseOnce you can no longer break muscle growth plateaus by increasing your calorie intake, that is when increasing your dose of exogenous anabolics is a reasonable strategy to deploy.Taper up your dose SLOWLY.This means as low as an additional 50-100 mg on top of your current weekly dosage, and that’s only after you have milked all the growth you can out of the last incremental dosage increase.Just like you taper up your weights in the gym, or your calorie intake in the kitchen, dosages should be titrated up slowly.After you increase your weekly dosage, milk all you can out of that incremental titration, and then once you plateau with that go back to step 1 and try increasing your calorie intake again.Rinse and repeat.Remember, the higher your doses are, the more your body will fight back, so you should milk the most muscle growth out of each incremental increase in your dosages possible before you increase your dosages again.I wish I had known this before I ever delved into the world of performance enhancing drugs, as I unnecessarily stressed my body out several times using dosages higher than I needed.How far can you take this strategy?Well, as far as you want based on your risk tolerance, up to a point.Anecdotally, most men will experience significantly diminished returns after passing 1500-2000 mg per week of steroids.Should you ever get this high to begin with?Probably not unless you are a competitive bodybuilder who has aspirations of becoming an IFBB pro.When Myostatin and other counterregulatory mechanisms in the body force you into a plateau, all you can do is increase your nutrient intake, or increase your dosages, and then milk that until Myostatin and other inhibiting factors elevate again to match that new level you have imposed on your body.These regulatory mechanisms will continue to elevate to match your intake, so how far you push this before cleaning out is up to you.I know some guys who will titrate all the way up to 2 grams of gear per week and 5000+ calories of food per day over the course of several months.I also know guys who look great who never go over HRT doses of Testosterone.What you deem overkill will be based on your health markers, risk tolerance, and personal goals.Go Off CycleEventually you will have to go off cycle to reset Myostatin (or lower your dose down to therapeutic TRT levels if you need to be on HRT).If you stay on a high dose of AAS for months, you will eventually plateau.Regardless of how advanced you are or how high your dosages are, once you decide you don’t want to push your body further with additional nutrients or drugs, you will need to go off cycle to lower the inhibiting mechanisms in your body back to baseline.Related

Topical Estrogen Cream For Hair Loss Prevention – My Experience And Review
I’ve been asked a few times about topical Estrogen cream for hair loss prevention.BiEstro-Care cream and Estrogel in particular.BiEstro-Care is a is a combination of 1 mg of natural Estriol USP and 0.25 mg of natural Estradiol USP per pump.I’ve also tried their Estradiol-only topical, Estradiol Care.Each full press of the pump provides approximately 0.1 mg of natural Estradiol USP in that topical preparation.I’ve also tried pharma grade Estrogel, which is an FDA-approved, bioidentical 17β-estradiol transdermal gel at 0.06% w/w strength.The hypothesis in the community is that the topical Estrogen cream will bind to Estrogen receptors in the scalp and produce a more conducive environment for hair loss prevention without going systemic as it remains localized on the scalp.Think of it like topical Minoxidil vs oral Minoxidil.The topical version doesn’t go systemic to the same degree, and still exerts significant pro-circulatory effects.[embedded content]Localized Estrogen Receptor ActivationOn paper, it is easy to extrapolate the potential benefit of being able to topically apply Estradiol or Estriol and get some sort of localized binding with a relative lack of systemic estrogenic activity.However, it just doesn’t seem to work like that in practical application.I noticed absolutely no difference on my hair growth or hair loss prevention, whatsoever.It’s also not very predictable in terms of pharmacokinetics in the body going through the scalp.Does Topical Estrogen Cream Promote Hair GrowthI can confirm that topical Estrogen cream on the scalp is very poorly absorbed and has minimal impact on hair growth, or the progression of androgenic alopecia.I checked my blood work via a high sensitivity assay (LC/MS-MS) and I was actually shocked at how poor the systemic absorption was through the scalp.If your goal is to try and maintain physiologic amount of systemic estrogen fulfilled via transdermal administration of topical Estrogen cream, you will likely be unsuccessful.The absorption through the scalp is extremely poor.I was drenching my head in this stuff to really test it out.Even when I had several milligrams of Estradiol cream on my head per day, my E2 levels were low.The hypothesized topical localized effect on Estrogen receptors also doesn’t seem to play out as we thought it may.I noticed no additional growth out of it, and feel that it is an overhyped growth agonist that may just do more harm than good.The most notable biomarker that changes with topical Estrogen cream on the scalp is Estrone, which goes through the roof.To date, I have never seen anyone actually get good results from topical E2 to begin with, and any cases of regrowth with its use were in cases where other therapies were used in conjunction with it.Anybody who deploys this as a form of monotherapy to prevent hair loss will be disappointed with their lack of results in my opinion.At the end of the day, preventing hair loss at the root of the issue just boils down to managing your overall systemic androgenicity relative to systemic estrogen levels.My Verdict On Its Efficacy For Hair Loss PreventionAs a growth promoting agent (what it would mainly excel at), I feel that is probably not even worth exploring to be honest.It certainly doesn’t seem to exert any antiandrogen-like effects at the androgen receptor either that would justify its use in my opinion.Related

Quad Injection | Why You Should NEVER Inject Your Quads
Never do a quad injection.There are other shot locations that are far better and I’m going to elaborate on why in this article.When you first get into this stuff and you’re trying to learn about proper administration technique the main shot locations you’ll see recommended are glutes, quads, and maybe delts.More often than not, guys are advised to pin their glutes or quads.Quads are the absolute worst place to pin in my opinion, and I advise you avoid it like the plague.While I haven’t researched about this specifically, purportedly there are more blood vessels in the quads, which can increase your likelihood of causing hemorrhaging and the build up of a hematoma.In addition, the quads are very nerve dense and it is far more likely that you will hit a nerve and cause muscle twitching during a quad injection.Also, if you get post-injection pain (PIP) in your quad, you severely inhibit your ability to function as you need to limp around on your leg and it can significantly impede simple day to day activities.Sure, you may have injected your quads hundreds of times with no problems.I had the same experience, I had perfectly sterile oil, perfect shot technique, and still eventually had a shot go awry.No matter how perfect your shot technique is, how sterile everything is, how perfect everything is laid out in your sequence of events for proper sterile administration, the likelihood that you will eventually have a shot that goes wrong in your quads I believe is much higher than with any other commonly used shot location.[embedded content]My Quad Injection MishapI’ve never had an infection.However, I did have one shot in my quad go awry several years ago.For no good reason at all, my quad started inflating with blood to the point where I needed to get it drained.There was no abscess, there was no infection.Clearly I pierced through something that resulted in hemorrhaging, and the build up of a hematoma in my quad.My leg swelled up with blood to the point where I couldn’t even bend it.My body would have eventually absorbed all that blood and been fine as there was no infection, but the pain was just too intense to deal with, and it would have taken months to drain naturally.So, I had a slit cut in my upper outer quad and drained the entire thing.There was so much blood and pressure built up that a projectile bloodstream smashed into the wall across the room after the slit was made in my quad.Immediately after I had instant relief, and then my leg healed up and was fine.This was using the exact same sterile testosterone I use for my TRT and there wasn’t even an infection.The technique was also perfect.There was no good reason for it, my leg just started hemorrhaging from the needle.Post-Injection PainEven if you don’t have a really bad shot that forces you to make a trip to the hospital, the likelihood is high that you will eventually encounter some level of PIP that cripples you to the point that you can barely walk.You depend on your legs to walk, and on top of that, it would be wise to avoid injecting areas that could visibly deform you in the first place should you ever encounter a complication or an infection.This is why I would not inject arms, delts, and after that ordeal, not quads either.It would be wise to avoid nerve dense muscle groups like the calves entirely as well.Unless you’re pinning 10+ cc’s of gear per week, there is no need to even rotate to your quads to begin with in the first place in my opinion.Choose injection locations that get sufficient blood flow and are the least important areas cosmetically should they get infected or have a complication arise.Also, they won’t prevent you from being able to walk properly if you get a bit of PIP.The Best Injection SitesThe two best injection sites in my opinion are the glutes and the ventro glutes.The ventro glute is an area that nobody seems to know about, but it is bar none the best injection site in my opinion.It is used most often in a clinical setting for intramuscular injections and can handle significantly more oil than most other sites, it gets a lot of blood flow, it is easy to reach if you are heavily muscled and inflexible (unlike the glute), and in general it seems to have the best overall risk profile out of all injection site options.The easiest way to find this spot is by leaning onto the leg on the side of your body that you’re trying to make the ventro glute jut out from.You’ll see the muscle pop out on the side when you put weight on that leg.For landmarks and a precise way to locate the ventro glute, I advise following the guide in the following video:[embedded content]The ventro glute is the ideal injection site in my opinion, and it is my main go-to spot for pinning my TRT.Steer clear of your quads.It is the absolute last place you should be pinning in my opinion, especially if you pin high volume.The higher volume you pin, the higher the likelihood of encountering some major issue during a quad injection.Even if that issue is just PIP, having PIP in your quads that makes you limp isn’t something you should ever have to deal with to begin with.Related
Can MK-677 Cause Brain Damage? | The Effects Of Chronic Ghrelin Exposure
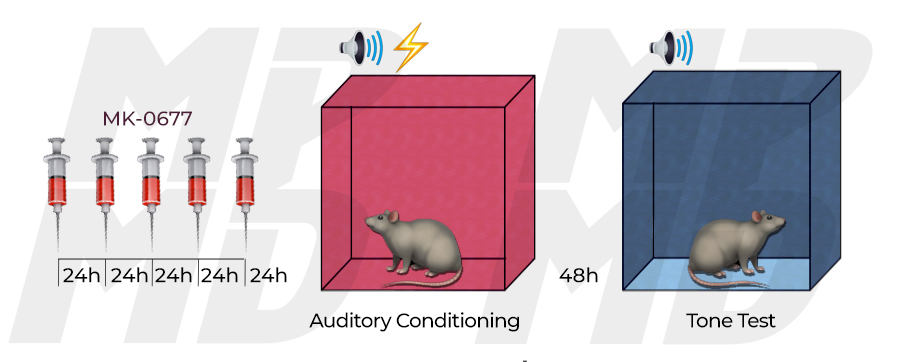
It is theorized in the community that MK-677 can cause brain damage via chronically elevating ghrelin levels in the body.Does this crossover to human use, and has it been observed to date?Well, there have in fact been links established between chronic ghrelin exposure and negative mental outcomes.I did cover this briefly in my original post.How applicable is this in humans though?[embedded content]Table of ContentsMK-677 Enhances Fear In RatsOne study on rats evaluated if MK-677 can cause enhanced levels of fear.There is evidence to support that one of the ways ghrelin is modulated is through exposure to stress.What this study intended to assess specifically was if rats would have a greater likelihood of experiencing fear and posttraumatic stress disorder (PTSD) when their ghrelin levels are artificially raised 24/7 with a ghrelin receptor agonist (MK-677).Rats were continuously administered MK-677 and frightened constantly, and their difference in response (MK-677 treated vs non treated) was assessed.The rats with chronic ghrelin elevation were found to have enhanced fear memory compared to baseline [R].Like I mentioned, there’s evidence to support that one of the ways ghrelin is modulated is through exposure to stress, and this study was able to stir up quite a bit of controversy in the community with its results showing a blatantly negative effect on the amygdala where the fear-enhancing effects of repeated ghrelin receptor stimulation seemed to be concentrated in.Ghrelin and growth hormone act together in the amygdala to enhance fear, at least in this rodent model.How Does MK-677 Work?If you don’t already know, ghrelin is the hunger hormone.As you would expect, ghrelin levels are high before meals, and low after finishing meals.This is how your body regulates its appetite and knows when to eat and when to stop eating.GHRP’s and GH secretagogues don’t just signal GH secretion, some also have a very significant effect on ghrelin.The most notable being GHRP-6 and MK-677.These are both notorious as appetite stimulating compounds.This is why peptides like GHRP-6, GHRP-2, and secretagogues like MK-677 cause such a drastic spike in hunger.When you use them, you’re basically tricking your brain into thinking you’re hungry when you otherwise may not be.Growth hormone is secreted by the somatotrophes of the anterior pituitary gland in multiple pulses each day.Growth hormone is released into the blood stream and then stimulates the liver to produce insulin-like growth factor-1 (IGF-1), which stimulates linear growth before epiphyseal fusion and also exerts several metabolic effects throughout life.After ingestion, MK-677 increases somatotrophe secretion of GH via signalling the pituitary gland to secrete a sufficient amount of growth hormone [R, R].The most common cause of GH deficiency in childhood is believed to be caused by a lack of adequate stimulation of the pituitary gland by hypothalamic GHRH, which is why something like Ibutamoren which can systemically increase IGF-1 levels for 24 hours with a single oral dose is very promising for potential clinical use [R].The likely mechanism of action following MK-677 administration is the activation of the ghrelin receptor by MK-677, with feedback by IGF-I preventing excess GH production [R].The mechanism of action through which MK-677 promotes GH secretion is comparable to growth hormone releasing peptides like GHRP-6, GHRP-2, Ipamorelin and Hexarelin, with GHRP-6 being the most similar in regards to the amount of ghrelin secretion that occurs post-administration.MK-677 does not stimulate a greater quantity of secretion events per day (number of GH pulsations), but rather it stimulates a greater total 24 hour GH production rate [R].In other words, Ibutamoren can substantially increase the strength of each GH pulsation that occurs in the body.Effects of treatment on 24-hour mean GH and IGF-1 and GH secretory dynamicsWas This Study Flawed?Rats chronically exposed to ghrelin were found to have enhanced fear memory compared to baseline.There is some confusion around exactly how this test was carried out, and the reality is that the rats weren’t getting MK-677 infused into their brains off the bat like many seem to think.In this study, rats were injected with 1ml/kg (i.p.).I.P. stands for Intraperitoneal injection, and is the injection of a substance into the peritoneum (body cavity).The peritoneum is the serous membrane forming the lining of the abdominal cavity.This is where MK-677 was first administered to evaluate whether increased activation of the ghrelin receptor is sufficient for enhancement of fear memory.After they established that activation of the ghrelin receptor is indeed sufficient for enhancement of fear memory, they then proceeded to infuse MK-677 directly into the basolateral complex of the amygdala to determine whether repeated ghrelin receptor activation in the basolateral complex of the amygdala is sufficient to enhance fear memory.Repeated intra-amygdala ghrelin infusions enhanced fear memory [R].Now, while this all paints a pretty bad picture for MK-677 at a first glance, keep in mind that this study also showed that a single injection of a ghrelin receptor agonist was not sufficient to enhance fear, and even chronic ghrelin receptor agonism did not alter locomotion, innate anxiety, or the expression of previously acquired fear memories [R].How Applicable Is This In Humans?In humans, MK-677 has been found to be well tolerated for over a year straight using 25 mg per day orally.Humans aren’t injecting this compound, and they certainly aren’t infusing it into their brains either.This finding has yet to be replicated in human trials, or even in anecdotal logs to date.With that being said, are they looking for this in the human data?Probably not, and obviously those using MK-677 recreationally aren’t getting brain scans before and after their use.You probably shouldn’t be chronically exposing yourself to ghrelin in the first place for years on end if you can avoid it.There are auto-regulating mechanisms in your body for a reason.It would be wise to err on the side of caution and cycle MK-677 if you are going to use it anyways, regardless of what the data may or may not imply.Even if there was no neurological risk, I would still advise cycling MK-677 if you are going to take it because of its effect on insulin sensitivity, which I think is a more immediate concern than any extrapolated claims about its effects on brain health.What I’d Be More Concerned With – Insulin SensitivityWe already know that MK-677 and exogenous GH can negatively impact blood glucose control, and we already know that poor blood glucose control is one of the main issues that cascades into the majority of health problems we see widespread nowadays.Chronically elevating your blood sugar with MK-677 is going to have a negative impact on your insulin sensitivity to some extent.Although several clinical studies found no change in blood glucose levels, there were a couple studies where MK-677 caused an elevation of fasted blood glucose levels and decreased insulin sensitivity [R, R].GH causes blood sugar levels to rise, which in turn requires the pancreas to work harder to compensate and release insulin to bring blood sugar levels back down to homeostasis.Chronic GH elevation can create chronic pancreatic stress in certain scenarios, which eventually can result in pancreatic beta cell degeneration, and insulin resistance.Chronic blood glucose elevation and pancreatic cell degeneration is what eventually leads to Type 2 Diabetes.Individuals with other lifestyle factors that contribute to insulin resistance as is (excessive carbohydrate intake, holding too much body fat, lack of exercise, etc.), or have genetic predispositions that increase their likelihood of Diabetes, could potentially end up pushing themselves over the brink and become Type 2 Diabetic with MK-677 or synthetic growth hormone usage.MK-677 can also cause reverse hypoglycemia in insulin resistant individuals.When MK-677 or GH raises blood glucose levels, this is autocorrected and regulated by the pancreas in healthy individuals.In insulin resistant individuals, MK-677 can cause reactive hypoglycemia, whereby sharp spikes in blood sugar can cause an exaggerated level of insulin secretion and glucose uptake into the cells, consequently crashing blood sugar and causing hypoglycemia [R].This poor endogenous regulation of blood glucose levels is typically indicative of some degree of insulin resistance in an individual.Signs and symptoms of reactive hypoglycemia may include hunger, weakness, shakiness, sleepiness, sweating, lightheadedness and anxiety.I believe that long-term MK-677 use will probably force you to to implement blood sugar control strategies that you wouldn’t have needed to otherwise.If you’re a borderline type II diabetic to begin with, and you throw MK into the mix long-term, that could easily push you over the border.For somebody completely healthy, you could potentially take yourself from completely healthy to like mildly insulin resistant if you deploy MK for years straight without breaks.Much like the same occurrence if you used a high dose of growth hormone for a long span of time, it would impede your blood glucose control to some degree.This doesn’t mean that you can’t use MK-677 or exogenous GH without developing insulin resistance, I’m simply asserting that you will likely have to keep a closer eye on your blood sugar, and may have to start incorporating certain strategies into your lifestyle that you may have not needed to otherwise to remain as healthy as possible while using it.Getting back to the effect MK-677 has on stress and fear, I don’t think it’s going to cause any notable mental degradation, and all of the clinical data and anecdotal logs seem to reinforce that.With that being said, throwing a wrench into your stress feedback loop may have deleterious outcomes that we are simply not evaluating with accurate metrics, and with that in mind, it would be wise to cycle MK-677, especially if it is being used for performance enhancement and not to treat a GH deficiency.If it is being used therapeutically for GH deficiency, obviously that is a different story.Monitor Your Glucose Control And Insulin SensitivityI think the more immediate concern when it comes to MK-677 is insulin resistance rather than the speculated neurological degradation that doesn’t seem to occur with its use in practical application at commonly used dosages in humans.We do know MK-677 has a notable impact on blood sugar not just in the long-term, but immediately following its first administration.In addition, the excessive amounts of ghrelin MK-677 causes the body to secrete will cause overeating in many individuals.The population is fatter than ever, and has already shown that they have horrible self-control when it comes to refraining from overeating.Add a ghrelin receptor agonist on top of that that literally tricks their brain into thinking that they are even hungrier and you can just imagine what the outcome of that would be for the average guy.In my opinion, this is the main concern with MK-677, not fear memory enhancement.If you are going to use MK-677 or exogenous GH, keep a blood sugar monitor on hand and keep a close eye on your fasting blood glucose levels, your blood glucose control post-meals, and incorporate lifestyle, diet, or supplement protocols that will prevent the excessive amounts of ghrelin and spike in GH/IGF-1 from impairing your health status.MK-677 has a lot of therapeutic promise, and can even enhance a performance enhancing protocol significantly if used correctly.Knowing how to minimize your risk profile while you use it though is critical and should be well thought out before you haphazardly start taking it without any prior research.Where To Buy MK-677Most companies do not third party test their products, nor do they have any satisfactory level of quality control whatsoever.I strongly advise that before you buy SARMs or MK-677 from a company online you thoroughly evaluate their track record, their third party test results, and how they are marketing their products in general.These Are My Current Trusted/Go To Companies For Third Party Tested 99%+ Pure MK-677:Science.bio – 10% off coupon code “DC10”Chemyo – 10% off coupon code “DC10”Amino Asylum – 20% off coupon code “DC20”Swiss Chems – 25% off coupon code “DC25”Disclaimer: The information included in this article is intended for entertainment and informational purposes only. It is not intended nor implied to be a substitute for professional medical advice. Prior to buying anything, check that it is compliant where you live with your current government laws.Related
Does Lactobacillus Reuteri ATCC PTA 6475 Probiotic Help Prevent Hair Loss? | My Review
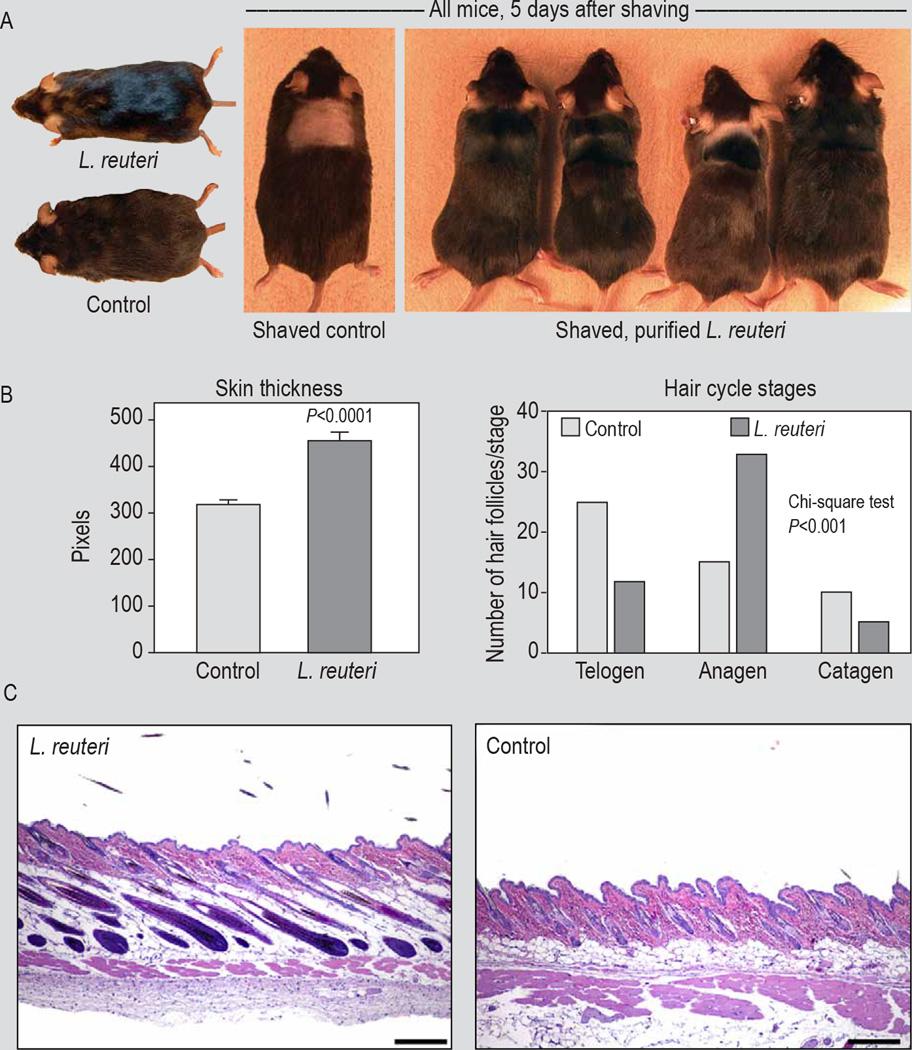
Lactobacillus Reuteri ATCC PTA 6475 is a strain that was hyped up in the community after an article was published called “Probiotic ‘glow of health’: it’s more than skin deep” [R].In the article, you can see that the mice that were fed with this probiotic strain experienced significantly better hair growth, and also exhibited a much more favorable ratio of anagen to telogen hair cycle stages.The majority of the article elaborates on how promising this probiotic strain is for hair growth, skin health, as well as overall health in general.Of course, I had to try this myself to see if there was any crossover in humans.[embedded content]My Experience With Lactobacillus Reuteri ATCC PTA 6475It was really hard to come across to find this exact strain.After digging for several hours, I found one company that sells it.I bought several months worth and took it diligently every single day.After using it for several months, I can confirm without a shadow of a doubt that it made no noticeable difference on my growth rate.Obviously, these images and results look really promising.When you see a mouse experience significant improvement in their hair growth with the only factor changed being this probiotic, you can’t help but assume this is very encouraging data.But, not everything in rodent studies translates into humans, and this is one of those cases where the probiotic I don’t think is worth adding to your regimen.My VerdictSave your money.The Lactobacillus Reuteri ATCC PTA 6475 probiotic strain doesn’t work well for hair loss prevention, if at all.With that being said, I’m not asserting that probiotics aren’t good for health.Good gut health does have some impact on levels of shedding, and potentially even androgenic alopecia in general.Inflammation and the inflammatory response in your scalp is obviously tied to your gut health at the end of the day.But, as far as the potential of this strain in particular inducing a unique growth effect that you wouldn’t get otherwise get, it just isn’t the case.Related
Oral Castor Oil For Hair Loss Review – My Experience And Others
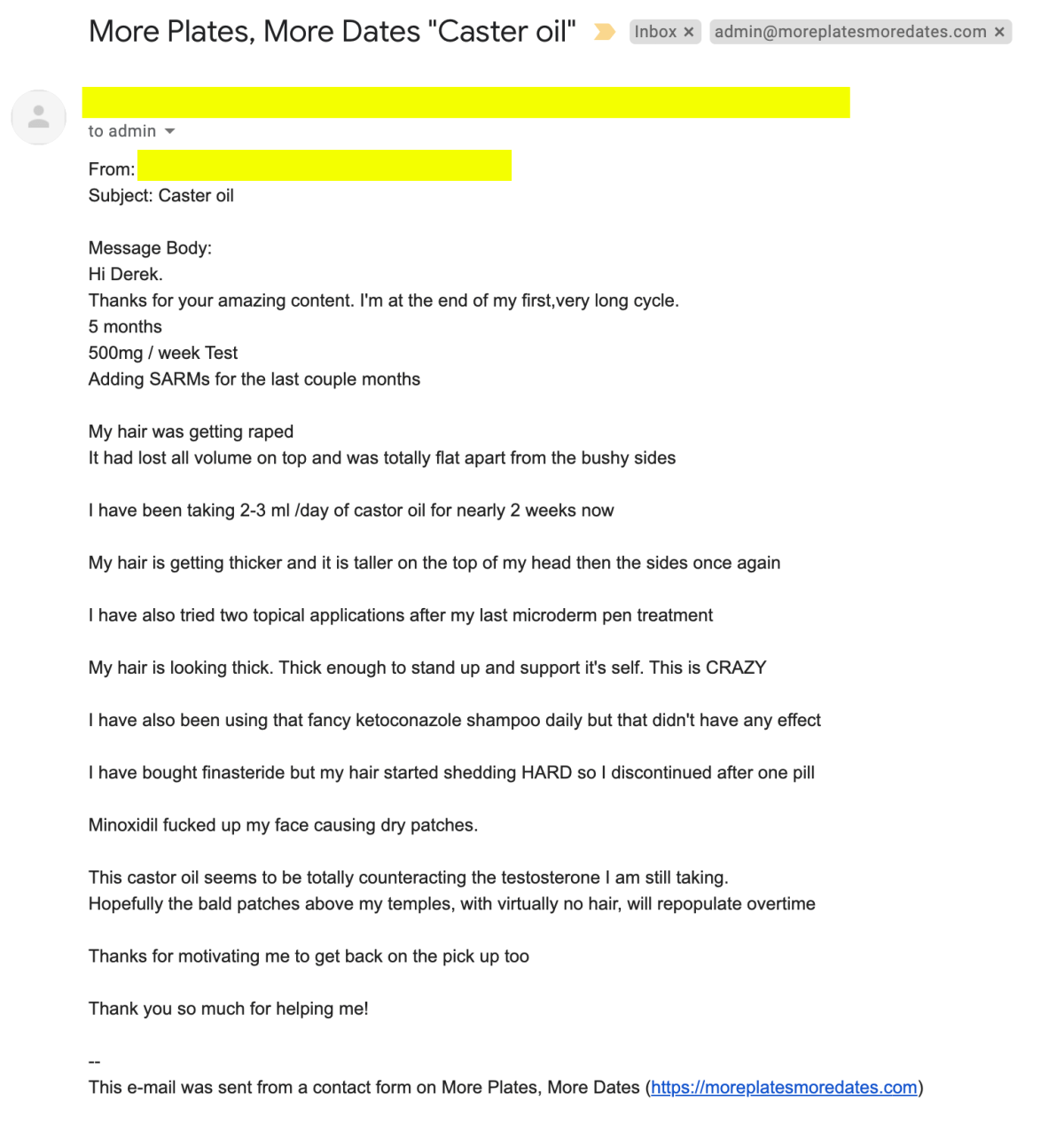
After I made my first oral castor oil for hair loss post a couple of months ago, I received hundreds of DM’s, private messages, YouTube comments, emails and tweets asking me to post an update.Well, here it is.After trying oral castor oil for hair loss for 2 months, I have concluded that it is an effective growth promoter, and is far more potent than topical castor oil.Is it more effective than Minoxidil as a growth promoter?No, however, it has a more tolerable side effect profile, is far cheaper, and provides results that are at least noticeable enough to justify it being worthwhile to explore further.There are VERY FEW compounds that can effectively promote a healthier rate of growth.The 2 most effective in my opinion are Minoxidil and MK-677.However, that doesn’t mean that they are sustainable long-term options for every one.With Minoxidil, circulatory issues can be a major problem for some, and with MK-677, glucose control and insulin resistance may pose an issue with long-term use.When considering the side effect profile for micro-dosing oral castor oil for hair loss, the worst side effect I have heard of so far is an upset stomach.Fortunately, if your digestive system doesn’t agree with castor oil, it is pretty easy to tell and immediately lower your dose, or discontinue your use.This is what I noticed personally using at least 1 mL per day for 2 months straight.[embedded content]Table of ContentsOral Castor Oil and Digestive IssuesWhen it comes to digestive issues, I’ve had none so far using as much as 1.5 to 2 milliliters per day.On a typical day I will just take 1 mL, but occasionally I will bump it up.There is no rhyme or reason to it, I just want to see how well I can tolerate up to 2 mL, but then some days I decide I probably don’t need that much and should stick with 1 mL.When I first started researching about oral castor oil for hair loss, there were a few guys who suggested that there is a point of diminishing returns once you hit 2 mL, and anything above that starts to put you into laxative territory.However, as more and more people have tried this, it seems more likely that there is a dose dependent improvement in results.So, there is a possibility that the more you can tolerate the better it will be for hair, but that will be individual dependent at the end of the day, and will only be determined via personal experimentation.Gut health is very sensitive.Some people can’t even drink a cup of milk without destroying their guts, and then some people have iron stomachs and can eat like crap and be fine.This is all individual dependent at the end of the day.I will probably try tapering up in the future to see how high I can get my daily dose without digestive distress.Despite the fact that I haven’t had any digestive issues as of yet, that doesn’t mean that it isn’t common.Over the past few months, I’ve spoke with dozens of individuals who have also tried oral castor oil for hair loss.While the majority of them found that it was effective, a handful of them discontinued because of gut issues.If you have compromised gut health as is (actually pretty common), adding castor oil on top of it probably won’t help.I would recommend optimizing your gut microbiome before you start taking oral castor oil, as it is fairly common to cause digestive distress, even at low dosages.In general, it seems like most are having fairly good outcomes with high levels of tolerability.One of my friends did actually discontinue because he thought that the quality of his sh*ts had started to show signs of digestive issues.However, he was taking 5 mL per day.In addition to that, his diet isn’t 100% on point.As mentioned, for me there’s been no difference, so far.I’m keeping it in my protocol for now and for the foreseeable future.A Glowing Review Sent In By A SubscriberI received this email shortly after posting my first video on castor oil and felt that it was worth including in this post.His personal information is redacted for privacy.Since I posted this article, a couple testimonials were commented on the YouTube video that I felt were worth including as well. My ResultsI do think that oral castor oil has positively impacted my growth rate to a notable degree.I definitely have to shave more often and get my hair cut more frequently now.I think my hair might even be getting a bit darker too, but that could just be me seeing things.It’s definitely growing quicker though without a doubt.Mainly what it seems to do well is offset the cosmetic look of hair loss.By improving your rate of growth relative to your rate of loss, you can create a more favorable ratio of hair follicles in the anagen phase relative to the catagen phase.While this isn’t directly preventing further loss be addressing the root of the issue, it can help you keep more hair on your head, and ultimately maintain a fuller head of healthy hair.If you’re a diffuse thinner, the benefits of oral castor oil will be even more evident as your issue more or less boils down to a horrible ratio of catagen to anagen activity.Keep in mind, if all you’re using is growth promoting agents like Minoxidil or oral castor oil, you’re fighting an upstream battle.The best strategy in my opinion is to lower your rate of loss as much as you can with compounds that address androgens directly, and then stack growth promoting agents on top of that.If you only use growth agonists like Minoxidil, you will eventually run into the inevitable problem where androgen induced miniaturization has progressed so much that the artificial increase in circulation you’ve induced with Minoxidil is no longer sufficient to offset your loss of hair density.Androgens are still wreaking havoc on your hair even when Minoxidil is in your system if you do not have something in your protocol that addresses androgens directly, or a part of the cascade that occurs as a consequence of androgens.Simply increasing circulation with a potassium channel opener is not going to be sufficient to stave off androgenic alopecia.I use the analogy of trying to row a canoe up a stream against the current to describe hair loss prevention.If you try to row against the current, you might be able to hold your ground for a while, but you’re fighting an uphill battle and the current doesn’t stop.Ideally what you would do is get the current to stop before you even get in the water (things like anti-androgens, 5-alpha reductase inhibitors, SARMs, Estrogen modulation, PGD2 inhibitors, etc.), and then get in the water and deploy your growth agonists as needed based on risk profile and tolerability (microneedling, oral castor oil, Minoxidil, growth hormone secretagogues, etc.).With that being said, growth promoting options that appear to be fairly low risk (like microneedling) make sense to deploy concurrently with whichever strategy you have in mind for tackling androgens off the bat.Castor Oil Long Term Safety ProfileTolerability as a laxative sheds light on the safety of micro-dosing oral castor oil for hair loss prevention in the short term, but in the long term, that remains to be seen.According to the Food and Agricultural Organization and World Health Organization, up to 0.7 milligrams per kilogram of castor oil per day is safe for men [R].Oral castor oil is also generally recognized as safe and effective for use as a stimulant laxative by the FDA.I’ve been using one milliliter per day on average, which is next to nothing by clinical standards.Women are given upwards of 60 milliliters in a single dose to induce labor [R].For constipation in adults, 15-60 milliliters in a single dose is commonly prescribed and generally recognized as safe [R].Minoxidil Vs. Castor Oil EfficacyMinoxidil is a more effective growth promoter than oral castor oil.However, oral castor oil seems to have a much better side-effect profile. In addition, this isn’t a one or the other choice that needs to be made.They can be used in conjunction with one another for an even better effect.When you compare them to one another, Minoxidil will win hands down in efficacy.However, oral castor oil will not cause you to shed horribly when you start it, and it also won’t cause a massive shed if you stop taking it.Both of which are huge limitations of Minoxidil.Minoxidil use backs you into a corner, and you have to think long and hard before you introduce it into your protocol as it can be very mentally taxing to make it through the initial shedding phase, and if you encounter intolerable side effects, you will have another shed when you stop using it.In addition, forcing the potassium channels to open more can have deleterious outcomes on the cardiovascular system, and it isn’t uncommon for individuals to report premature aging of their skin with Minoxidil as well.Those are two massive limitations of its use that oral castor oil does not seem to have.Don’t get me wrong, Minoxidil can be a great addition for some individuals, but it is certainly not a low-risk treatment and should be approached with caution.The only limiting side effect of castor oil that I’m aware of as of now is its gastrointestinal effects that may not be tolerable for all individuals.Other than that, it’s extremely cheap, seems to have a very favorable risk profile, and is at least in the same ballpark as Minoxidil in regards to efficacy.That is more than you can say for any other growth promoting agent out there with a stamp of safety approval by the FDA.The only other growth promoting agent I can think of off the top of my head that’s formidable to Minoxidil and oral castor oil is MK-677, or literal growth hormone injections.But, is that really a long-term sustainable practice just for hair density?Ideally, you don’t want to potentially put yourself in a state of compromised blood glucose control just so you can get a better growth rate on your head.When it comes to growth promoting agents, I believe that oral castor oil is one of the most cost-effective and well-tolerated options there is for a beginner.Oral Castor Oil Vs. PGE2 Applied To The ScalpThe reason oral castor oil works is the Ricinoleic Acid in it that increases PGE2 in the body as discussed in my first post.Logically, one would assume that using straight PGE2 instead of oral castor oil would be even more effective for hair growth, as the end goal of using castor oil in the first place is increasing PGE2 in the body.In practical application though, oral castor oil actually seems to work better than literal topical PGE2.In the past, I would microneedle my scalp with the Derminator (a microneedling device) set at 1.5 mm and then apply straight PGE2 to my scalp afterwards.In theory, this seems like a great idea to tip the scales in the body to a more favorable PGE2 to PGD2 ratio.After a lot of experimentation, I believe that oral castor oil is superior for a few reasons.The first being that PGE2 is extremely expensive.Castor oil is literally 1/1000th the price (maybe even less).In addition, PGE2 is measured in such small quantities (micrograms) that trying to avoid overdosing it while still getting sufficient scalp coverage is near impossible.By using castor oil, you give your body the ability to regulate how much PGE2 it converts, rather than overloading your system with a massive spike in PGE2 that could potentially have deleterious consequences long term.Also, the results I got from oral castor oil were better than what I experienced with diligent PGE2 applications.Now, at the end of the day, this all still stems back to androgens causing this whole cascade of events.The whole process can be mitigated just by addressing the Testosterone and DHT at the beginning.But, obviously for people that aren’t willing to manipulate their hormone profile, or aren’t willing to implement certain things that they perceive as too experimental, things like castor oil can be excellent additions to a protocol.And for those who are willing to manipulate their hormones a bit more, or use higher risk treatment options, castor oil is still something I see as a potentially low risk addition to help solidify a strong, comprehensive regimen.Where Does Castor Oil Fit Into A Hair Loss Prevention Protocol?Something that will be asked is how oral castor oil compares to traditional treatment options.Castor oil operates via a totally different mechanism of action and cannot be compared to things like Finasteride, or Dutasteride, or RU58841, or even PGD2 inhibitors.The compound accomplishes what its meant to do, but it will not replace anti-androgens, or other compounds meant to do completely different things in the body.At the end of the day, a comprehensive protocol should address all factors, or address the root of the issue early enough in the cascade so sufficiently that nothing else matters.You can’t compare a PGE2 agonist to an anti-androgen, so keep that in mind.Where To Buy Food Grade Castor OilYou want to buy 100% castor oil, not Jamaican black castor oil.It’s clear and a pale yellow color.Food/Pharma grade (USP or BP) is ideal as it ensures a high enough standardization of Ricinoleic acid.Ricinoleic acid is the component of castor oil that boosts PGE2 and we care about.NOW Solutions Castor Oil is third party tested and meets our criteria for a high quality Castor Oil, and is also what I use personally.Related

NPC TEXAS LEGENDS CHAMPIONSHIPS – Mens Physique
NPC TEXAS LEGENDS CHAMPIONSHIPS – Mens Physique

NPC TEXAS LEGENDS CHAMPIONSHIPS
NPC TEXAS LEGENDS CHAMPIONSHIPS DALE PIERCE OVERALL BODYBUILDING WINNER Men’s