Human growth hormone (HGH) and steroids—proven performance-enhancers that were once the fuel behind the high-powered offenses of Major League Baseball—are increasingly becoming outcasts in the sports world. But while their effectiveness (and potential unfairness) make them dirty words for stat geeks, HGH and steroids continue to emerge as tools in the pain care toolbox.
A recent study in The Journal of Pain Research looked at the effect from injections of recombinant HGH and testosterone to the painful and dysfunctional areas in patients with chronic lower back pain. Pain ratings and self-rated functional outcomes were assessed.
Thus far, long-term outcomes for HGH and testosterone injections for lower back pain (LBP) and chronic lower back pain (CLBP) have been mixed. An ongoing problem is the lack of a standardized definition for CLBP, with some studies considering it pain beyond 3 months, while others simply refer to “pain lasting longer than the expected healing time.”
The best results are typically for lumbar facet joint injection and physiotherapy treatment. Facet and sacroiliac joint denervation have demonstrated successful moderate-duration pain relief when the joint is determined to be the source of pain, but this treatment destroys some nervous tissue and, according to the study authors, “does not directly address pathology or modulate pain from areas other than the joint.”
In the case study presented in The Journal of Pain Research, 60 participants suffering from CLBP were given an experimental treatment. Those who responded favorably to diagnostic blocks were given injections of HGH and testosterone in the treated areas, along with some follow-up manipulation and impairment-based exercises. Of the 60 patients selected, 39 completed all aspects of the study. Those patients receiving the intervention reported a significant decrease in pain ratings (P<.01) and a significant improvement in self-rated scores on the Oswestry Disability Index (ODI) (P<.01)
Within the ODI results, 41% of the participants reported a greater than 50% improvement. There was also a statistically significant improvement in the participants’ reporting of symptoms, with an overall self-reported improvement of 74%, including 92% reporting a 50% or greater improvement (P<.001).Of those patients who did not complete all aspects of the study, one was due to pain related to the injections, while the others were for nonstudy factors.
“The intervention appeared to be safe and the results provide a reasonable expectation that the intervention would be beneficial for a population of individuals with chronic nonradicular lower back pain,” the study authors note.
The next step is a randomized, controlled trial for which controls for psychosocial and other variables can be instituted—a noted limitation of this study.
Use of localized human growth hormone and testosterone injections in addition to manual therapy and exercise for lower back pain: a case series with 12-month follow-up
Objective: The objective of this case series was to investigate the feasibility and safety of a novel method for the management of chronic lower back pain. Injections of recombinant human growth hormone and testosterone to the painful and dysfunctional areas in individuals with chronic lower back pain were used. In addition, the participants received manual therapies and exercise addressing physical impairments such as motor control, strength, endurance, pain, and loss of movement. Pain ratings and self-rated functional outcomes were assessed.
Study design: This is a case series involving consecutive patients with chronic lower back pain who received the intervention of injections of recombinant human growth hormone and testosterone, and attended chiropractic and/or physical therapy. Outcomes were measured at 12 months from the time of injection.
Setting: A community based hospital affiliated office, and a private practice block suite.
Participants: A total of 60 consecutive patients attending a pain management practice for chronic lower back pain were recruited for the experimental treatment. Most participants were private pay.
Interventions: Participants who provided informed consent and were determined not to have radicular pain received diagnostic blocks. Those who responded favorably to the diagnostic blocks received injections of recombinant human growth hormone and testosterone in the areas treated with the blocks. Participants also received manipulation- and impairment-based exercises.
Outcome measures: Outcomes were assessed at 12 months through pain ratings with the Mankowski Pain Scale and the Oswestry Disability Index.
Results: Of the 60 patients recruited, 49 provided informed consent, and 39 completed all aspects of the study. Those patients receiving the intervention reported a significant decrease in pain ratings (P<0.01) and a significant improvement in self-rated Oswestry Disability Index scores (P<0.01). In addition, in the Oswestry Disability Index results, 41% of the patients demonstrated a 50% or greater change in their disability score. Of the subjects who withdrew from the study, one was due to the pain created by the injections and nine were for nonstudy factors.
Conclusion: The intervention appeared to be safe and the results provide a reasonable expectation that the intervention would be beneficial for a population of individuals with chronic nonradicular lower back pain. Due to the design of the study, causality cannot be inferred, but the results do indicate that further study of the intervention may be warranted.
Keywords: lumbar, sacroiliac joint, manual therapy, injections, pain management, rehabilitation
Background and significance
The efficacy of injection therapy for low back pain (LBP) can be regarded as having mixed results and limited long-term clinical benefit.1,2 Likewise, the evidence is mixed regarding exercise and manual therapy for the management of chronic LBP (CLBP).3–5 Reviews have indicated generally similar, but mixed short-term responses for facet injections and physiotherapy treatment.6 Lumbar facet joint injection is recommended as the first line of treatment prior to lumbar facet radiofrequency denervation, with similar results obtained from both treatments.7,8
A problem in investigating CLBP is the lack of agreement of the definition of CLBP, with the definition including 12 weeks of pain, pain lasting longer than the expected healing time,9 and pain lasting beyond 3 months.10 The “socio-professional” factors and psychosocial dysfunction are also confounding factors in regard to investigating interventions for mechanical LBP. It appears that depression may hinder the long-term outcome for lumbar pain managed through radiofrequency denervation of the facet.11 Licciardone et al12,13 describe a predominance of somatic dysfunction in the lower back and pelvic girdle area in individuals with CLBP, indicating that for many, the problem may well be multifactorial and includes somatic components.
While facet and sacroiliac joint denervation have demonstrated successful moderate-duration pain relief when the joint is determined to be the source of pain, the intervention requires destruction of nervous tissue and does not directly address pathology or modulate pain from areas other than the joint.14 Clearly, delineation of new beneficial treatments for LBP, and particularly CLBP, would be welcome. A significant volume of patients with LBP are reported to present with structural pain involving tendon, ligament, and joint degeneration and dysfunction.15–17 If the etiology of the ongoing pain and dysfunction includes both movement impairments and soft tissue degenerative change, interventions to address both impairments and pathology should prove to be more beneficial than addressing one problem alone.
Exercise and manual therapy are intended to address motor control, movement impairment, and dysfunction, with any change in the soft tissues occurring through remodeling, which requires extended time and adherence to lifestyle changes and interventions.18–20 An alternative intervention that facilitates tissue remodeling would be expected to shorten and improve the rehabilitation process. Localized injections with recombinant human growth hormone (rhGH) and testosterone are conceivable candidates as treatment options for this purpose. Both are endogenous anabolic hormones that stimulate protein synthesis and have demonstrated marked benefits on early wound healing.21–23
The systemic effects of rhGH have classically been attributed to the production of its sister molecule, insulin-like growth factor (IGF)-1, in the liver. However, rhGH has also been found to stimulate protein synthesis independent of IGF-1, working locally as well as systemically.24–28 In addition, protein synthesis is facilitated by the presence of anabolic hormones. A synergistic effect of testosterone and rhGH on protein synthesis has been repeatedly demonstrated.25–28 With this potential influence on protein synthesis, the injection of rhGH and testosterone into degenerative tissue may possibly lead to the formation of new collagen and its maturation into new connective tissue at the injection site, although this mechanism could create contractures and unwanted scarring as well. It is hypothesized that this type of injection will lead to strengthened collagen and improvement in the biomechanical properties of chronically degenerated, damaged, and painful tissue, such as ligament and joint capsule. In conjunction with the injections, rehabilitation involving manual therapy and exercise would be expected to positively influence movement behavior, motor control, and remodeling of the neuromuscular system and dense connective tissue, while possibly preventing contractures, but this is highly theoretical.
The potential mechanisms for the injection to be effective include both the needling of the tissue and introduction of the rhGH and testosterone. The needling of the fibro–osseous junction during the injection of these two anabolic hormones produces an injury that possibly stimulates macrophages into action. Macrophages have been found to be a rich source of diverse growth factors that can direct repair and remodeling after injury29,30 and are thought to play an integral role in successful healing processes, including wound debridement, initiation of neovascular growth, and stimulation of fibroblast proliferation and protein synthesis.30–32 Both rhGH and testosterone may exert an effect on the macrophage as an activating factor, acting directly on receptors, independent of IGF-1.33,34 In addition, macrophages have been found to recruit stem cells to the wound area, which may possibly further stimulate the healing process.29 Further information on the stimulation of tissue healing and growth with rhGH and testosterone has been discussed elsewhere.35–46
Based on the potential for injections to promote the regeneration of connective tissue and rehabilitation to improve function, the combination exhibits potential to lead to improved outcomes in CLBP. To investigate the feasibility and the potential for the synergistic benefit of these interventions for LBP, a case series using the novel treatment of rhGH and testosterone injections combined with rehabilitative therapy for CLBP patients was undertaken. The purpose of this case series is to demonstrate the feasibility of a novel injection for CLBP and that the technique can be accomplished safely. Once the protocol is determined to be safe and potentially effective, studies to investigate clinical outcomes through randomized controlled trials and to discern the mechanism of action can be conducted, for which controls for psychosocial and other variables can be instituted.
Methods
Study design
The study represents a case series of sequential participants who met the inclusion criteria. The purpose of the case series was to determine the feasibility of conducting a future randomized controlled trial. This 12-month follow-up case series was undertaken in a private pain management clinic. While the participants were receiving the injections, they were also seen in community chiropractic and physical therapy clinics for rehabilitation that focused on manual therapy and stabilization/motor control exercises.
The study was approved by the Institutional Review Board of Roper St Francis Healthcare, Charleston, SC, USA. Data were monitored by a Data Collection Site Monitoring Board and Adverse Experience Reporting Committee. A board-certified, hospital-affiliated anesthesiologist/pain management physician administered the initial examinations and injections under fluoroscopy. Patients participating in the case series were also examined by and received impairment-based manual therapy and exercise programs administered by chiropractors and/or physical therapists.
Participants
Sixty consecutive adult participants, aged 18 years or older with nonradicular CLBP were sequentially recruited as a convenience sample during the interval of June 2009 to June 2011. Inclusion and exclusion criteria are listed in Table 1. Participants were followed up at 1 month, 3 months, 6 months, and 12 months following the last injection. Following a standardized clinical examination by both the anesthesiologist/pain management physician and the chiropractors/physical therapists, a specific diagnosis of pain secondary to lumbar facet, sacroiliac joint, and/or ligament dysfunction was determined with local anesthetic injections performed under fluoroscopic guidance. Complete or near complete (90%) resolution of pain was considered diagnostic for nonradicular pain and was used to determine the location for the study injections.47,48 All participating patients had a negative straight leg raise, prone knee-bend test, and Slump test for radicular pain reproduction. Three participants presented with postoperative pain syndrome following fusion surgery. An additional six patients had lumbar surgery without fusion, without resolution of symptoms. Participants had received a range of management strategies including trigger point, sacroiliac joint, and lumbar facet injections, radiofrequency facet denervation, pharmacological pain management, and chiropractic and physical therapy. The interventions were not consistent across participants. Participant demographics are listed in Table 2.
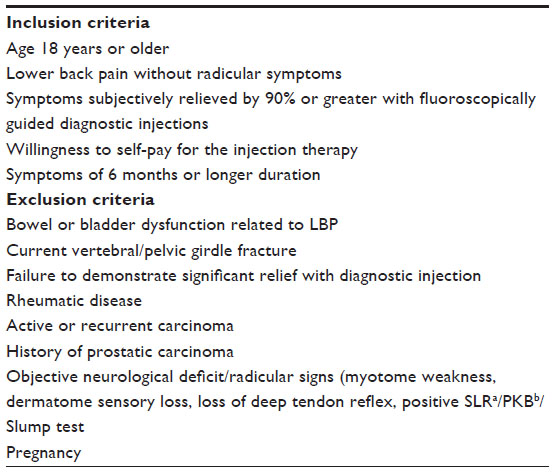 |
Table 1 Inclusion and exclusion criteria |
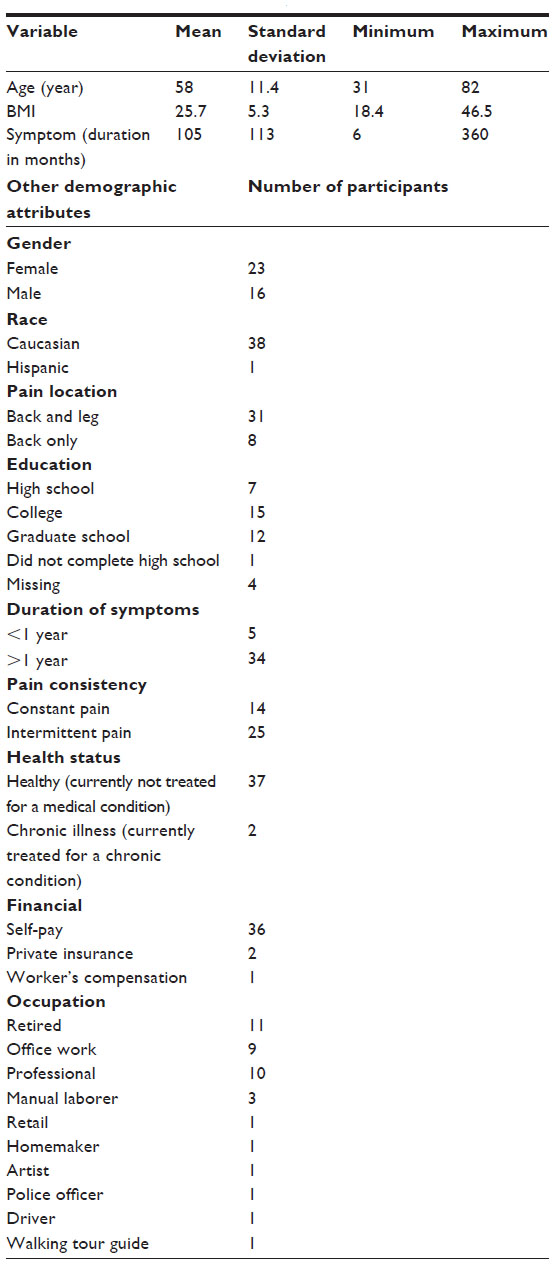 |
Table 2 Demographics for participants beginning the study (n=39) |
Interventions
Each participant received rhGH (Sandoz rhGH; Sandoz International, Holzkirchen, Germany; 1 mg/10 cc volume), testosterone (12.5 mg for females, 25 mg for males, per 10 cc volume), 5 cc of 1% preservative-free procaine, and 0.9% NaCl to a total volume of 10 cc with injections performed at the fibro–osseous junction of symptomatic areas (ligament, tendon, and capsule) under fluoroscopic guidance at 2–4-week intervals, and they averaged four to five injections in total. Approximately three 10 cc syringes were administered at each injection visit. An individualized rehabilitation program, including joint manipulation and exercise therapy, was designed for each participant by the participating chiropractors and physical therapists (Table 3). After the injection therapy was completed, participants were followed for 12 months. The participants attended therapy until discharged with a home exercise program. No attempt was made to discern if the participants continued to exercise after discharge from therapy.
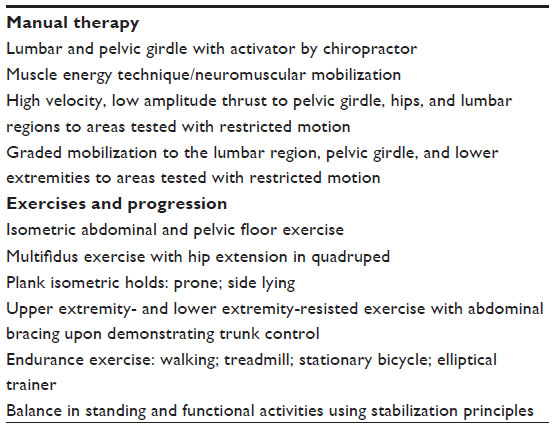 |
Table 3 Interventions used with rehabilitation and manual therapy |
Outcome measures
The primary outcomes were determined by the patient’s pain rating from 0 to 10 (Mankowski Pain Scale [MPS]) and the Oswestry Disability Index (ODI). The MPS is a 0–10 pain rating scale that links verbal descriptors of the intensity of the symptoms to a numerical value. The MPS has been shown to be a valid and reliable tool for pain measurement, as compared to the Faces Scale, the Visual Analog Scale, and the Numeric Rating Scale.49 The minimal clinically important difference for the change score has not been determined, but it has reported as two points for the Numeric Rating Scale.
The ODI is a condition-specific self-rated disability tool. The minimal clinically important difference for the ODI has been reported to be between 6 and 14 points.50–54 In addition, a 50% change in the ODI has been described as a rigorous outcome measure regarding LBP.55 As a secondary outcome, participants reported overall percent change in presenting symptoms.27,56 In addition, testosterone levels (total testosterone) and HGH levels (measured as IGF-1) were measured at study intake in order to determine if a correlation exists with the baseline blood levels and the change in outcome measurement scores.
Analysis
Due to the lack of significant skewness and the absence of outlier/extreme values in the frequency distributions of the outcome variables, parametric means testing was utilized to determine the statistical significance of changes from study entry to 12-month follow-up. Pearson’s correlation coefficient R2 was used to test correlations between entry blood level IGF-1 and testosterone with the three outcome variables at 12-month follow-up.
Results
Out of all recruited patients, eleven elected to not enter the treatment program. Of the remaining 49 qualified participants, all provided informed consent to enter the study. All phases of the study including the 12-month follow-up were completed by 39 of the 49 qualified patients (80%). Of the ten who did not complete the study, three were noncompliant with the treatment protocol, six had surgical procedures, and one felt the injections were too painful (Table 1). Of the surgical procedures, three were not related to the back pain problem. A laminectomy and two fusion procedures were performed on the other three participants. At the 12-month follow-up, statistically significant mean decreases in pain severity (change of 3 points) and disability (change of 22.2 points) were found (Table 4). Within the ODI results, 41% of the participants reported a greater than 50% improvement. There was also a statistically significant improvement in the participants’ reporting of symptoms, with an overall self-reported improvement of 74%, including 92% reporting a 50% or greater improvement (P<0.001).
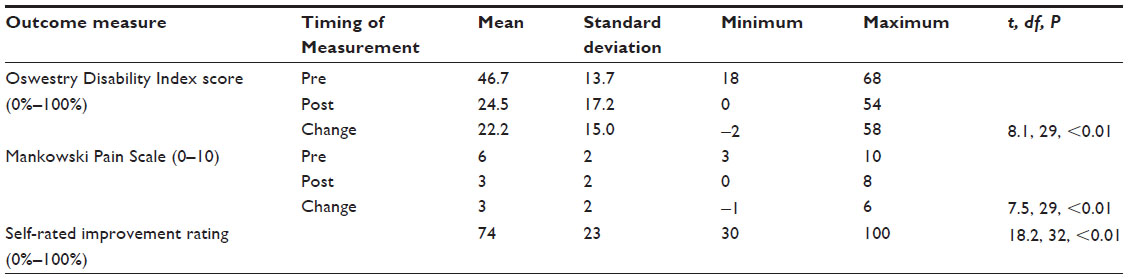 |
Table 4 Change scores in outcome measures and statistical significance |
There were no significant correlations between study entry IGF-1 or testosterone levels and changes in the three outcome variables at 12-month follow-up (R2 linear ≤0.01). While one participant dropped out of the study due to the pain associated with the injections, no other adverse reactions related to the study were reported during the course of the treatment or at the follow-up sessions. Nonstudy-related medical conditions (Figure 1) led to five individuals dropping out of the study.
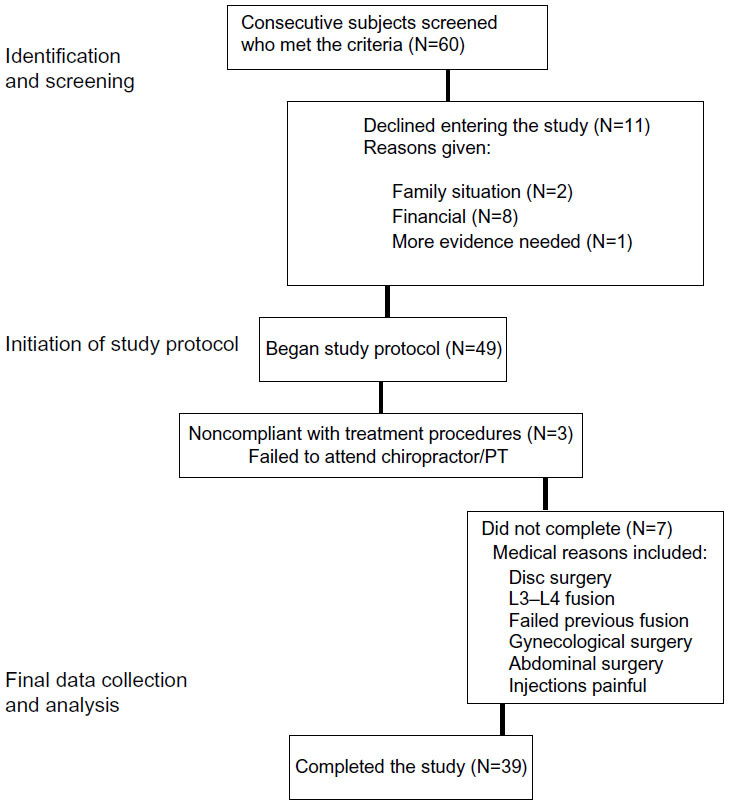 |
Figure 1 Study participation flowchart. |
Discussion
Participant outcomes demonstrate a potential for rhGH and testosterone injections in conjunction with manual therapy and exercise to play a role in improving function and relieving pain related to CLBP. This finding occurred in a group of patients where previous heterogeneous interventions, including trigger point, sacroiliac joint, and lumbar facet injections had produced suboptimal results. The case series results were achieved using a novel injection therapy along with impairment guided exercise and manipulation (Table 3). Three of the participants who started the study were dropped out due to the need for surgical intervention for their back pain: one who had a failed previous fusion; one who suffered an acute lumbar herniation and underwent a lumbar discectomy; and one who underwent lumbar fusion surgery. These individuals’ data are not included in the outcomes.
A recent randomized controlled trial comparing facet steroid injections with radiofrequency denervation8 reported on two groups of patients with CLBP who received either facet injection or radiofrequency denervation. At a 6-month time point, the mean ODI for the injection group and the radiofrequency denervation group were found to be similar. Lilius et al57 reported no difference in the outcome between placebo and steroid facet injections. In this case series, the magnitude of the change in the ODI scores was much larger than that found for steroid injections or denervation. In addition, this case series emphasized the combination of injections with rehabilitation that was based on each participant’s impairments.
Manual therapy has conflicting evidence for the management of LBP, but it does appear to be somewhat effective for acute LBP.58,59 A recent review reported that there is no clear evidence to the benefit of manipulation versus exercise for the management of CLBP.60 The present case series examined the participant outcomes with intervention with a combination of a novel injection therapy, manual therapy, and exercise. The nature of the case series does not allow for any analysis of the interaction between interventions, or the specific role any of the interventions played in influencing the results. The results do support the development of future randomized controlled trials that are designed to examine these factors and others that may influence the outcomes.
Limitations
Psychosocial variables were not measured nor analyzed in this case series. While it is recognized that psychosocial variables play a major role in many individuals with CLBP, we felt that it was not possible to control for these variables in a case series of this nature. The chief purpose of this case series was to demonstrate the safety for the use of rhGH and testosterone for what was determined to be mechanical LBP.
One subject dropped out of the study due to the pain created by the injections, and no medical adverse responses were reported. Participants were told that they would be sore and that they may have increased pain for a few days following the injections, and all but one appeared to be accepting of this.
While all participants had failed to improve with previous management strategies, including various injections and surgery for some of the participants, it can still be argued that impairment-based rehabilitation rather than the injections may have had a major influence on the outcomes. Due to the nature of this case series, it is not possible to assign cause and effect to any of interventions offered. The fact that all but one of the participants completing the study reported consistent or intermittent pain for greater than 1 year prior to the intervention, and that one participant reported pain for greater than 6 months, arouses suspicion that a possible interaction between the injections and rehabilitation is of benefit, but this is unknown at this time and needs to be investigated in future studies. Only 14 (36%) participants reported continuous pain with 25 (64%) of the subjects reporting intermittent, yet chronic pain. It is possible that the timing of the measurement could influence the results if a patient were having a “good” phase of the disorder. When completing the ODI, the participants rated their function over the past week, which should help resolve this issue to some degree.
Conclusion
In summary, the combination of rhGH and testosterone injections in conjunction with rehabilitative therapy consisting of joint manipulation and exercise therapy may hold promise for a number of patients with CLBP, helping a greater number of individuals than injections, manual therapy, or exercise alone. We currently hypothesize that the injection therapy leads to the stimulation of collagen formation resulting in strengthening of the ligaments and other dense connective tissues. The remodeling of these tissues may be a causative factor leading to long-term benefits with this treatment.
This case series has demonstrated that this line of investigation is safe, with 80% of the participants completing the study, and only one dropped out due to the injection procedure, which was due to local pain during the procedure. This form of treatment has demonstrated that it has potential to help what may be a large subgroup of patients with CLBP who have no satisfactory treatment options to recommend. To our knowledge, this is the first study using localized rhGH and testosterone injection therapy in patients with CLBP and demonstrates the potential benefits in a long-term continuation. The results of this case series support the development of randomized controlled trials comparing the use of placebo injections versus rhGH and testosterone injection therapy, with and without impairment-specific rehabilitation.