After reviewing the molecular weight of some of the most promising SARMs developed, I theorized that they could potentially be prepared in a topical solution for hair loss prevention.
As you probably already know, Selective Androgen Receptor Modulators (SARMs) are a class of androgen receptor ligands that bind to androgen receptors and exert tissue selective anabolic effects with a relative lack of androgenicity when compared to traditional anabolic steroids.
The end goal of their continued development is more or less to create the ultimate anabolic agent that can completely offset tissue loss as a result of musculoskeletal degenerative diseases, with a complete absence of androgenic activity in the body.
While certain SARMs are closer to reaching this goal than others, the perfect SARM has yet to be developed.
However, that doesn’t mean that the SARMs currently developed cannot be leveraged in some capacity for a variety of potential applications.
As alternatives to oral SARMs, topical SARMs may be a promising area of research in the fight against hair loss.
This article highlights the reasons why I believe there is such therapeutic promise in topical SARMs for hair loss prevention.
Role Of Androgens In Causing Hair Loss
Despite there being a cascade of events that lead to hair loss, the presence of too many androgens is ultimately what causes follicular miniaturization.
However, the effects of exogenous androgens on the human body will inevitably vary between individuals due to several dependant factors in this cascade.
As a rule of thumb, raising androgen levels via exogenous androgens will generally initiate or accelerate hair loss for someone who is hair loss prone.
Unfortunately, anabolic steroids will unavoidably bring along some degree of concurrent androgenic activity.
Our natural endogenously produced steroids are not an exception to this, and the androgen load in the body needs to be addressed in some capacity to attenuate, or even reverse hair loss.
Standard Treatments For Hair Loss: Finasteride And Dutasteride
Finasteride and Dutasteride are medications designed to treat hair loss by inhibiting the enzymatic process responsible for DHT production.
This means that they are not anti-androgens that bind to androgen receptors, but rather they prevent the body from converting testosterone into the much more androgenic metabolite dihydrotestosterone (DHT) by inhibiting the enzyme 5-alpha reductase.
A 5 mg dose of Finasteride per day will inhibit approximately 70 percent of the body’s systemic DHT, in comparison to 0.5 mg Dutasteride; which inhibits 90 to 99 percent of the body’s systemic DHT.
For most individuals, androgenic activity caused by DHT will be minimized after Dutasteride serum concentrations have peaked in the body, as there will simply be barely any DHT left.
However, even with a high dose of Dutasteride, scalp DHT levels may not be diminished enough to completely deprive the tissues of DHT, and there is a substantial concurrent spike in scalp testosterone levels as a result of the blockade created at 5-alpha reductase.
Not only is there potential for residual scalp DHT, but you if you rely on a 5-alpha reductase inhibitor as a form of hair loss prevention monotherapy you will still have a significant amount of testosterone unaccounted for in your body that still has its own inherent androgenic activity.
I’ve posted a video on this before, where I review my over one year long experiment with Dutasteride where I lowered my DHT to undetectable levels and increased my testosterone levels into borderline supraphysiological territory.
The inherent androgenicity of testosterone was still substantial enough to progress my androgenic alopecia.
In fact, I still had all the characteristics of androgenic activity:
- facial hair growth
- body hair growth (albeit notably reduced, which is to be expected)
- high libido
- morning wood and good erectile quality
- hair loss
In contrast to 5-alpha reductase inhibitors, a compound that reduces androgenic activity in the scalp by effectively targeting the androgen receptors would be more efficacious in staving off further hair loss progression.
This is what prompted the development of anti-androgens.
Transgender Hormone Therapy (Male-To-Female) For Hair Loss Prevention
During the process of male-to-female gender transitioning, one of the first things doctors would do is prescribe estrogen or an estrogen analog to crush endogenous testosterone levels while increasing feminine hormones.
They may also introduce anti-androgens to the protocol to further reduce the amount of androgenic activity in the body.
One of the side effects of gender transitioning via anti-androgen and estrogen therapy is significant scalp hair regrowth, and complete reversal in even some of the most extreme cases.
In some instances, men with nearly slick bald heads have grown back pre-puberty heads of hair via this kind of protocol.
While this is clearly the most extreme method of reversing androgenic alopecia, you can’t argue with the results it produces in individuals who feel the risk/reward is worth it, or simply desire to become more feminine.
Certain non-steroidal anti-androgens that interact with androgen receptors are designed to compete with testosterone and DHT for androgen receptor binding, while other steroidal anti-androgens work through slightly different mechanisms, albeit still working around the biological target of endogenous androgens (the androgen receptor).
For the sake of not overcomplicating this section with too much scientific jargon, I’m going briefly summarize the pharmacodynamics of the two most commonly used anti-androgens in the hair loss prevention community, and elaborate on how SARMs may stack up to them.
Bicalutamide
Bicalutamide is a non-steroidal anti-androgen that is recognized for its affinity to androgen receptors, thus preventing testosterone and DHT from binding and transcribing their effects in tissues.
Bicalutamide is a highly selective competitive silent antagonist of the androgen receptor, and is often utilized in androgen deprivation protocols, both clinically and experimentally.
A common feature of pure anti-androgens, such as Hydroxyflutamide and Casodex (Bicalutamide), is their relatively weak binding affinity for the androgen receptor, 50–100 times less than that of Testosterone [R].
On paper, it doesn’t seem like Bicalutamide would be very effective at preventing hair loss because of its weak binding affinity.
However, the typical prescribed dosages of Bicalutamide are high enough that so much of the drug gets into the system that it essentially overpowers testosterone and DHT for androgen receptor binding.
The logic behind this protocol is basically that the drug is poor at what it is designed to do, and for it to work it needs to be dosed extremely high until there is just so much of it circulating in the body that it overpowers testosterone and DHT by sheer volume.
The half-life of Bicalutamide is 5-10 days as well (depending on single vs. continuous dosing), consequently allowing serum concentrations of the drug to accumulate far more over time.
By creating a blockade of the androgen receptor, bicalutamide prevents the negative feedback androgens would normally create via the hypothalamic–pituitary–gonadal axis (HPG axis) in men.
As a result of this, luteinizing hormone (LH) spikes in the body as the body recognizes a need to produce more androgens.
After LH spikes, the gonads produce more testosterone, and more of that testosterone 5-alpha reduces into DHT, as well as aromatizes into estrogen.
150 mg Bicalutamide per day in men has shown to increase testosterone levels by 59-97%, increase estrogen levels by 65-146%, as well as increase DHT, SHBG and prolactin to a less significant degree.
This significant spike in estrogen will often lead to estrogenic side effects during Bicalutamide monotherapy.
Gynecomastia is a very common occurrence during Bicalutamide monotherapy.
Cyproterone Acetate
In contrast to the non-steroidal anti-androgen Bicalutamide, the steroidal anti-androgen Cyproterone acetate works by suppressing testosterone production directly, as well as competing for androgen receptors.
Cyproterone acetate is one of the first anti-androgens developed, but it is still one of the most effective to date for hair loss prevention.
With that being said, it has also shown to be one of the most side effect ridden compounds used for this purpose.
Cyproterone acetate was originally clinically deployed to “treat” hypersexuality and sexual deviation.
It was also used to delay precocious puberty.
When puberty begins before age 8 in girls and before age 9 in boys, it is considered “precocious puberty”.
As cyproterone acetate was used both in full grown men as well as pre-pubescent children, the conflicting findings in its pharmacodynamics have led to differing conclusions on how it works in the body, but for the sake of this article being about full grown men preventing hair loss, we will obviously be evaluating the clinical data on full grown men.
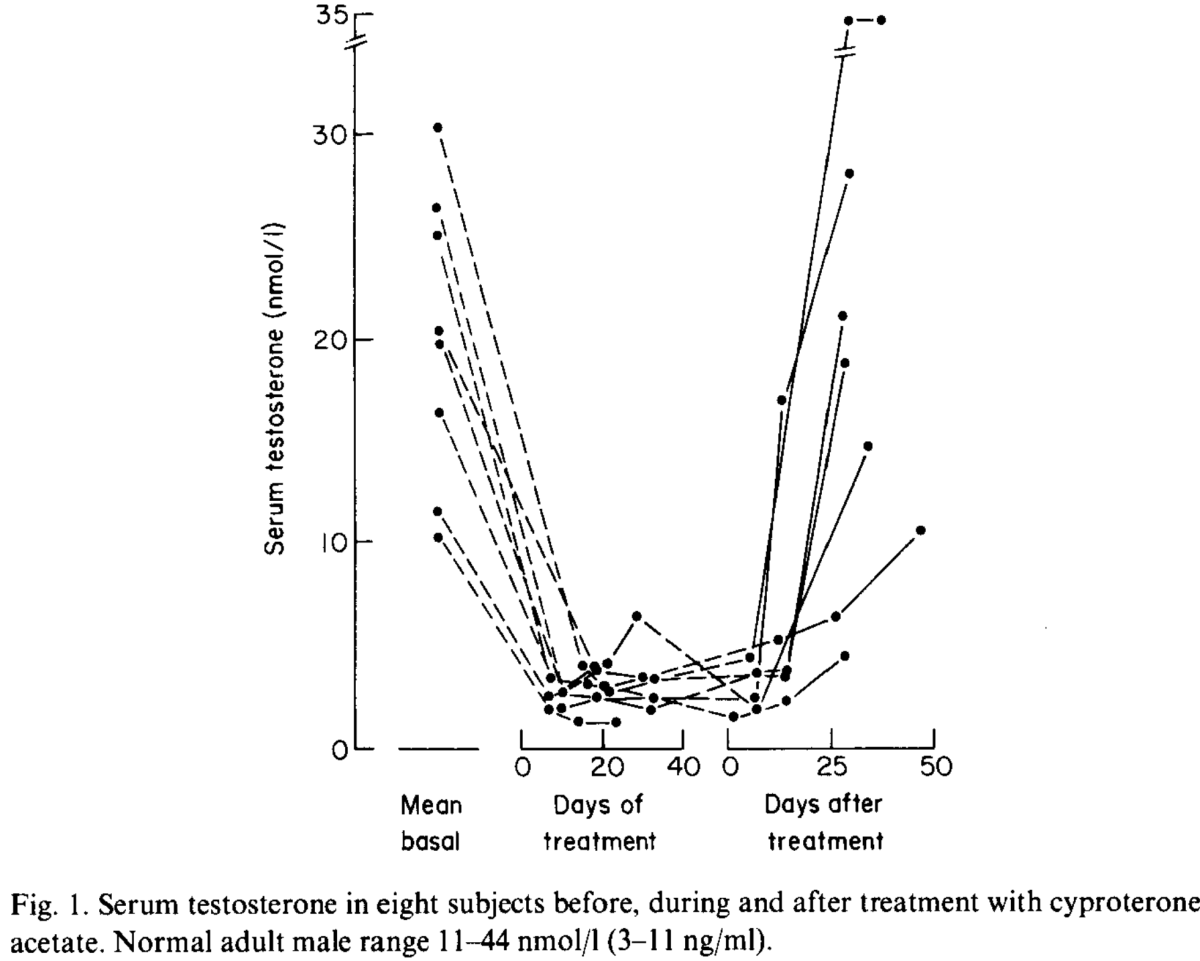
Cyproterone acetate causes a prompt drop in LH and FSH levels, and consequently a massive drop in testosterone levels.
In a study conducted on healthy male sexual offenders, dosing 50 mg cyproterone acetate twice daily caused testosterone levels to fall to subnormal levels within 1 week [R].


Cyproterone acetate has the highest anti-androgenic activity of any other clinically used progestin.
Despite it having a fairly weak binding affinity when compared to DHT and testosterone, Cyproterone acetate works similarly to Bicalutamide in that it accumulates during daily dosing because of its 1.6–4.3 day half-life, and also is dosed high enough clinically to increase serum concentrations high enough to a point whereby it can effectively compete for AR via sheer volume.
In addition, because Cyproterone acetate significantly reduces testosterone production (and by extension DHT production) via its progestogenic activity, there are less endogenous androgens for Cyproterone acetate to compete with for AR as it accumulates, consequently making it very effective at displacing androgens at AR and inducing systemic anti-androgen activity.
Cyproterone Acetate Vs. Bicalutamide
Steroidal anti-androgens have largely been replaced now by non-steroidal anti-androgens clinically, but cyproterone acetate and spironolactone are still commonly used in the management of feminizing hormone therapy.
Cyproterone acetate is more effective at reversing hair loss than Bicalutamide anecdotally, but also comes with a significantly elevated risk profile associated with its use.
Maintaining Masculinity Vs. Your Hair
While oral anti-androgens certainly work to reduce androgenic activity in the scalp, they also will often cause a variety of undesired side effects.
Aside from the actual health concerns in regards to hepatotoxicity, musculoskeletal degeneration, and more, the main thing we are going to focus on is the effect anti-androgens have on your literal manhood.
Expectedly, anti-androgens can cause feminization, loss of libido, erectile dysfunction, as well as muscle and bone loss.
Now, like I mentioned, non-steroidal anti-androgens like Bicalutamide are substantially better in this regard, whereby they will not cause musculoskeletal degeneration, will maintain relatively normal sex hormone levels, and do not have many of the drawbacks of steroidal anti-androgens [R].
However, that doesn’t mean that they are ideal, as they can still throw off the balance of androgens to estrogens in the body and prevent you from improving your body composition.
Anything inhibiting testosterone from binding to androgen receptors in muscle and bone and transcribing anabolic effects will get in the way of your body composition goals at the end of the day.
Inhibiting DHT and testosterone from binding to androgen receptors systemically will also impede countless physiologic processes that are facilitated via endogenous androgens in the body.
This isn’t a flaw of the drug necessarily, as it is doing exactly what it was designed to do.
However, androgen deprivation does not complement most of our goals as men, nor does it complement our health and quality of life.
We want androgen deprivation in the scalp only, with no alteration of our systemic hormones or health markers.
Obviously this is easier said than done, or else we would already have a topical anti-androgen available that stays localized, has a higher binding affinity than DHT, and has no systemic absorption.
This compound does not exist, so we have to make do with our current pharmacology and understanding of pharmacodynamics.
Oral Anti-Androgens Vs. Topical Anti-Androgens
Many would question why we don’t just use Cyproterone acetate or Bicalutamide topically to achieve this.
The reason why these fall short as topical treatments essentially boils down to the fact that their binding affinity is poor, and their success as anti-androgens is largely achieved via their accumulation in the body systemically.
When it comes to topical treatments, we don’t want something with a week long half-life, as it will start to accumulate in the body and cause systemic anti-androgen effects.
The ideal compound would be something that has a short half-life, a high binding affinity for androgen receptors, and acts as a highly selective competitive silent antagonist in the scalp exclusively.
The closest we have come to this so far is RU58841, with CB-03-01 showing therapeutic promise as well despite having a much lower binding affinity.
A compound that does not convert to deleterious metabolites systemically is also advantageous, as there will unavoidably be some level of systemic absorption with any molecule that is small enough to penetrate the stratum corneum after topical application.
While current topical anti-androgens commercially available do work for some individuals, there are limitations to each which I have delved into before.
There is no perfect treatment at the moment, but in this article I elaborate on something I feel is worth further exploration when it comes to creating a strong localized androgen receptor blockade with as minimal of a systemic impact as possible.
How Anti-Androgens Are Related To SARMs For Hair Loss
At the end of the day, how does this all intertwine with SARMs?
The bodybuilding community, the hair loss prevention community, and the research between them actually intersects in many ways that are commonly overlooked.
I first realized the therapeutic promise of SARMs in a hair loss prevention capacity when I saw someone stop their hair loss cold turkey with the SARM S4 and exogenous Estradiol.
What many don’t realize is that non-steroidal SARMs like S4 were synthesized using the chemical structure of traditional anti-androgens like Bicalutamide as their backbone.
The most promising SARMs exhibit binding affinities several times higher than these anti-androgens, and I feel are an extremely promising area of untapped research for hair loss prevention.


Some SARMs at certain dosages have shown to be as anti-androgenic as compounds like Bicalutamide and Hydroxyflutamide, more anti-androgenic than Finasteride, but with the benefit of actual tissue selective anabolic activity in muscle and bone.
Basically, some SARMs can prevent hair loss better than Finasteride, as well as traditional anti-androgens, all while allowing supraphysiological muscle growth.
The reason this is possible is that most SARMs have much higher binding affinities than traditional anti-androgens and can be far more effective at competing with endogenous androgens for AR binding and activation.
In addition, because they are tissue selective, once they bind to androgen receptors, they induce anabolic activity in muscle and bone with a relative lack of androgenicity in other tissues like the prostate and scalp.
I detail how this works further in one of my older articles called “Do SARMs Cause Hair Loss? | Can SARMs Prevent Hair Loss“.
Oral SARMs also lower SHBG and can have a suppressive effect on endogenous androgen production at high enough dosages (and even low dosages with some SARMs).
Through this suppression, SARMs can lower the androgen load in the body even further.
With long-term use, certain SARMs may suppress endogenous testosterone production enough that the use of estrogen alongside the SARM becomes a necessity if aromatization is no longer satisfactory to maintain healthy estradiol levels.
This presents an interesting scenario whereby androgen levels can be crushed to nearly undetectable levels via a non-steroidal SARM, and the additional negative feedback provided by the exogenous estradiol being added to the protocol to maintain therapeutic estrogen levels.
The end result of this is essentially a heavy duty anti-androgen protocol that can maintain significantly more muscle mass than what is possible via traditional androgen deprivation therapy.
However, oral SARMs obviously have their limitations as suppression of endogenous androgens is going to result in decreased libido, drive, and overall masculinity.
While many who use traditional anti-androgens don’t care about this as they simply want the most efficacious way to nuke their hair loss, there are going to be many individuals who want to minimize the systemic impact of any treatment they deploy to keep their hair.
This is where I believe there is therapeutic promise in topical SARMs.
Difference Between Topical SARMs For Hair Loss And Topical Anti-Androgens
SARMs and anti-androgens are both effective at inhibiting gene transcription via androgen receptor competition.
By competing against endogenous androgens for androgen receptor binding, topical anti-androgens like RU58841 and CB-03-01 are effective at preventing hair loss completely for some individuals with mild hair loss, and moderately effective at providing at least a decent foundation of protection for some individuals with more aggressive hair loss.
One limitation of topical anti-androgens is that they work in a dose-dependent manner, but can wreak havoc if they get systemic.
As I showed earlier with Bicalutamide, the higher volume of drug present, the more difficult it is for testosterone and DHT to bind to vacant androgen receptors.
With anti-androgens its not as simple as increasing the dose until it works though, as topical solutions will go systemic to some extent, and the more drug you introduce to your system, the more anti-androgen activity you will get systemically.
For someone with aggressive hair loss, chasing the volume approach with topical anti-androgens to overwhelm the endogenous androgens present in the scalp may lead to significant systemic side effects before adequate androgen receptor competition to prevent hair loss is even achieved.
SARMs on the other hand will have a negligible impact on endogenous androgen production when trickling into the system in trace amounts, and will not induce anti-androgen activity in muscle and bone even if a substantial amount of it does get into the bloodstream.
| SARMs | Anti-Androgens | |
| Comparable Binding Affinity To Testosterone For Androgen Receptors | SOME | SOME |
| Transcription Of Anabolic Affects | YES | NO |
| Transcription Of Androgenic Affects | MINIMIZED | NO |
| Side Effects To Systemic Introduction | MINOR | MAJOR |
How SARMs May Complement Finasteride Or Dutasteride
As DHT has a binding affinity higher than all SARMs, and significantly higher than all anti-androgens, if sufficient AR competition could not be achieved locally via a SARM or anti-androgen to stave off androgenic alopecia, then a 5-alpha reductase inhibitor could then be looked at as a potential adjunct treatment to use concurrently.
By dropping systemic DHT levels via 5-alpha reductase inhibition, competing for AR becomes significantly easier for us as we have compounds at our disposal that are actually comparable to testosterone in binding affinity.
The 500 Dalton Rule For The Skin Penetration Of Chemical Compounds And Drugs
The molecular weight of a compound must be under 500 Dalton to allow skin absorption [R].
Larger molecules cannot pass the corneal layer.
The Dalton is used as a unit of molar mass, especially in biochemistry.
1 Da (dalton) = 1 g/mol.
The Most Promising SARMs For Hair Loss Prevention
Taking S4 (Andarine) as an example, you can see that the molecular weight is 441.4 g/mol [R].
Because S4 has a molecular weight of 441.4 daltons, it can pass the corneal layer and work to some extent topically.
I’m using S4 as an example simply because it seems to be the most hair safe SARM of all to date via oral administration, and is also the only SARM I have seen used topically so far.
It is also the only SARM I’ve seen used orally in conjunction with exogenous estradiol for over a year straight so far with great success and no notable deleterious effects to liver enzymes or other health markers that are commonly impaired with high dosages of oral SARMs.
With that being said, S4 isn’t without its potential issues itself.
SARMs are still uncharted waters, but there are several that have been well tolerated in a clinical setting at dosages several times higher than what we would be using for hair loss prevention, or even for muscle growth in a bodybuilding context in a few token scenarios.
While S4 has shown to be the most promising SARM in a hair loss prevention context to date, I am confident that other alternatives with improved binding affinities, high tissue selectivity, and high tolerability clinically in actual human subjects would likely result in similar positive outcomes if the dosing was nailed down.
For example, LGD-4033 has a molecular weight of 338.25 daltons and has shown to be well tolerated in humans at dosages as high as 22 mg per day orally [R].
It has also binds to the androgen receptor with an extremely high affinity (Ki of ~1 nM), which is superior to every other SARM tested on humans with comparable tissue selectivity.
In addition, a preclinical rodent model showed that it has greater than 500-fold selectivity of muscle tissue to prostate when compared to testosterone.

A greater than 500:1 anabolic to androgenic selectivity would make LGD-4033 the most tissue selective SARM to date.
However, in practical application, LGD-4033 seems several times more androgenic than S4, although it is also several times more anabolic milligram for milligram.
Some individuals even report hair loss with LGD-4033 use.
Context is key here though, as the individuals reporting hair loss are using dosages 10x higher than the dosage being evaluated in humans clinically, and it is not clear whether this is telogen effluvium or actual androgenic alopecia progression even in these mega-dosing cases.
This is what I mean by the dosing needs to be nailed down with these compounds, as haphazard overdosing could easily lead to unexpected androgenic activity, or induce telogen effluvium via a significant shift in endogenous hormones.
There is no SARM that is completely devoid of androgenic activity, so dose response needs to be carefully assessed when experimentation is done with these compounds.
Anabolism as a Systemic Effect of Topical SARMs for Hair Loss
One of the limitations of anti-androgens is that when they go systemic they can induce anti-androgenic activity in other tissues.
SARMs on the other hand bind to androgen receptors and induce tissue selective anabolic activity.
So, the theory here is that we can potentially use a lower dose of a SARM topically than we would need with an anti-androgen, and achieve a substantial anti-androgenic effect via a much lower dosage, and even if it were to go systemic to some extent, then the worst that happens is we get some anabolic activity in muscle and bone.
In theory, it sounds great, but SARMs will still suppress endogenous androgen production to some extent, lower SHBG, and potentially induce some hepatic stress when systemic.
However, the degree to which this occurs should be much lower than what occurs with traditional anti-androgens.
This is all theoretical at the end of the day, as SARMs may not even compete for AR activation in the scalp.
However, anecdotally via oral administration it seems fairly obvious that they do in all tissues in the body, despite having “selective” action.
If a topical anti-androgen works, then a topical SARM should work in a similar way.
SARMs are essentially just chemically modified anti-androgens with better binding affinity and anabolic activity after all.
Efficacy Profile Of Topical SARMs For Men Wanting To Retain Masculinity
For many men, hair is a huge part of their identity and plays a massive role in looking good.
Unfortunately, we’ve been put in a position biologically where the more androgens in our body, the more expedited our hair loss progression will be, and all effective anabolic agents have some level of androgenicity.
So, in a perfect world, we would be able to utilize SARMs (or something like SARMs) to selectively occupy androgen receptors in the scalp, and leave the rest of the body alone.
Topical SARMs For Hair Loss Prevention: A Viable Long-term Strategy?
While SARMs are still very new, there are already SARMs with comparable binding affinities to testosterone that have shown to have no virilizing effects in women at fairly high dosages orally.
Topically, we may be able to achieve more localized action on androgen receptors and minimize the systemic impact in the body.
I believe there are better ways to manage hair loss than blindly crushing androgen levels with primitive medications.
SARMs may or may not be the answer, but they are certainly a step forward and could very likely be used effectively as a form of monotherapy in some users, or as an adjunct treatment alongside tried and true compounds that do a significant amount of the heavy lifting, and then let a SARM clean up the mess leftover.
Are SARMs perfect?
No, they aren’t.
However, some of the SARMs currently developed may already have more therapeutic promise for some individuals than traditional anti-androgens used for hair loss prevention.
At the very least, they are worth exploring more in this context, and I believe are potentially a more progressive way to go about handling excessive androgenic activity via AR activation in the scalp.
In addition, injectable SARMs are a new area I’m researching that may also have therapeutic promise as well.
How To Create A Topical SARM
The ideal scenario would be that we mix a SARM into a topical solution that has shown to not only be very tissue selective with a high binding affinity, but has also shown to be well-tolerated in humans in a clinical setting with no deleterious outcomes, and then apply that solution topically to bind locally to androgen receptors and compete with testosterone and DHT for AR activation.
Standard vehicles (the carrier solution you mix the compound in for topical application) should work similarly to anti-androgens.
My guess is that a 70% ethanol/30% propylene glycol vehicle would suffice.
A PEG 400 mixture may be a useful alternative vehicle for those with intolerance to propylene glycol, or those with vehicle-dependent contact allergy to SARMs in either propylene or hexylene glycol [R].
Adding a bit of DMSO or daily microneedling with a short length pretreatment may need to be incorporated for absorption for those with less permeable skin.
What concentration the solution should be remains up in the air and will need to be determined via experimentation.
Following the dosage outlines used in a therapeutic setting, we can get a well-tolerated starting point.
For example, with LGD-4033, orally it has a tissue selective anabolic effect at dosages as low as 0.1 mg per day, and has shown to be well-tolerated as high as 22 mg per day.
The most notable clinical trial on LGD-4033 utilized 0.5 mg, 1 mg and 2 mg orally for 12 weeks.
LGD-4033 exhibited encouraging safety and tolerability, and there were no drug-related serious adverse events in the study [R].
A good starting point would be 0.5 mg LGD-4033 per day topically, with the dosage titrated up accordingly based on dose-response.
The only SARM I’ve seen used topically to date is S4.
As S4 does not have any human data, we had to design the protocol based around anecdotal findings and extrapolated clinical data on rodent models.
Anecdotally, orally administered S4 does not induce night vision side effects until around 30-50 mg per day.
A topically administered dosage of 25 mg per day produced a very quick reduction in sebum in the scalp, which is a very obvious marker of reduced androgenic activity.
Scalp itch was also severely decreased, with no notable side effects.
Notably, the individual who I oversaw who did this experiment gets horrible side effects from every single hair loss prevention compound he has tried.
He’s one of the unfortunate ones who gets brutal 5-alpha reductase inhibitor side effects, systemic anti-androgen side effects with topical anti-androgen use, and even severely impaired sleep with PGD2 inhibitors.
The fact that he had no issues with topical S4 was very promising, and piqued my interest in the area even more (which is partially what has led me to my current injectable SARMs experiment I am conducting on myself).
Does that mean this is a viable long-term strategy?
That remains to be seen with further experimentation.
To be clear, this is still a theoretical approach to topical hair loss prevention, and is geared mostly towards individuals who have experienced negative side effects with 5-alpha reductase inhibitors, RU58841 and CB-03-01.
Where To Buy SARMs
Most companies do not third party test their products, nor do they have any satisfactory level of quality control whatsoever.
I strongly advise that before you buy SARMs from a company online you thoroughly evaluate their track record, their third party test results, and how they are marketing their products in general.
These Are My Current Trusted/Go To Companies For Third Party Tested 99%+ Pure SARMs:
Science.bio – 10% off coupon code “DC10”
Chemyo – 10% off coupon code “DC10”
Amino Asylum – 20% off coupon code “DC20”
Swiss Chems – 25% off coupon code “DC25”
Disclaimer: The information included in this article is intended for entertainment and informational purposes only. It is not intended nor implied to be a substitute for professional medical advice. Prior to buying anything, check that it is compliant where you live with your current government laws.